GLP-1 Receptor Agonists: A Comprehensive Review
- By Isaac
GLP-1 Receptor Agonists: A Comprehensive Review
GLP-1 receptor agonists (GLP-1RAs) represent a class of medications that mimic the action of glucagon-like peptide-1 (GLP-1), a natural hormone involved in regulating glucose homeostasis. Originally developed as adjunct therapies primarily for adults with type 2 diabetes mellitus (T2DM), these agents have demonstrated potential benefits in areas such as glycemic control, weight management, and cardiovascular risk factors. This review provides an overview of their background, mechanisms of action, therapeutic applications, clinical evidence, challenges, and future directions, drawing from peer-reviewed sources. These statements have not been evaluated by the Food and Drug Administration. This information is for educational purposes only and is not intended to diagnose, treat, cure, or prevent any disease.
Mechanisms of Action
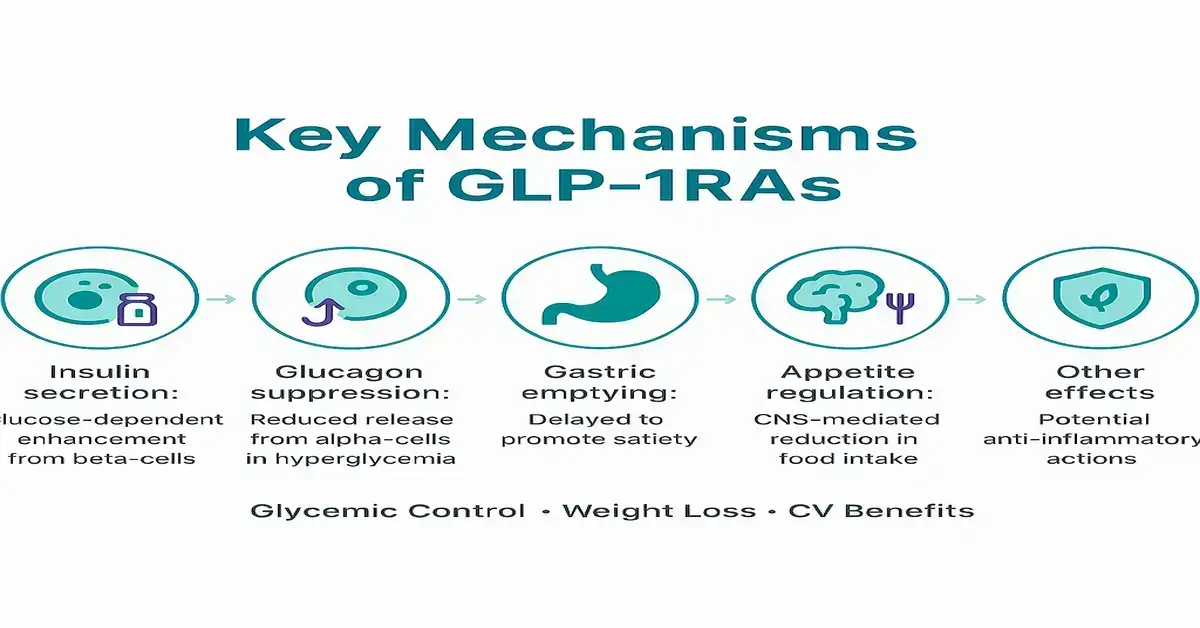
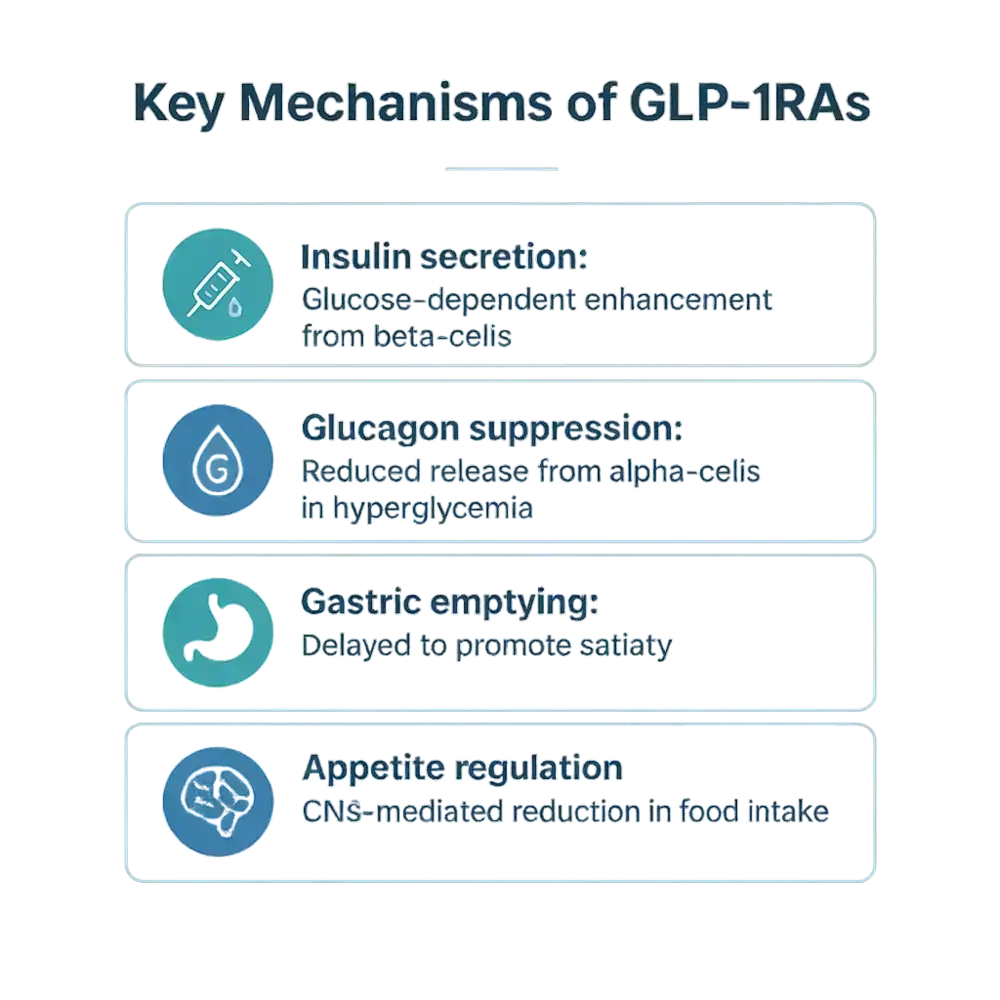
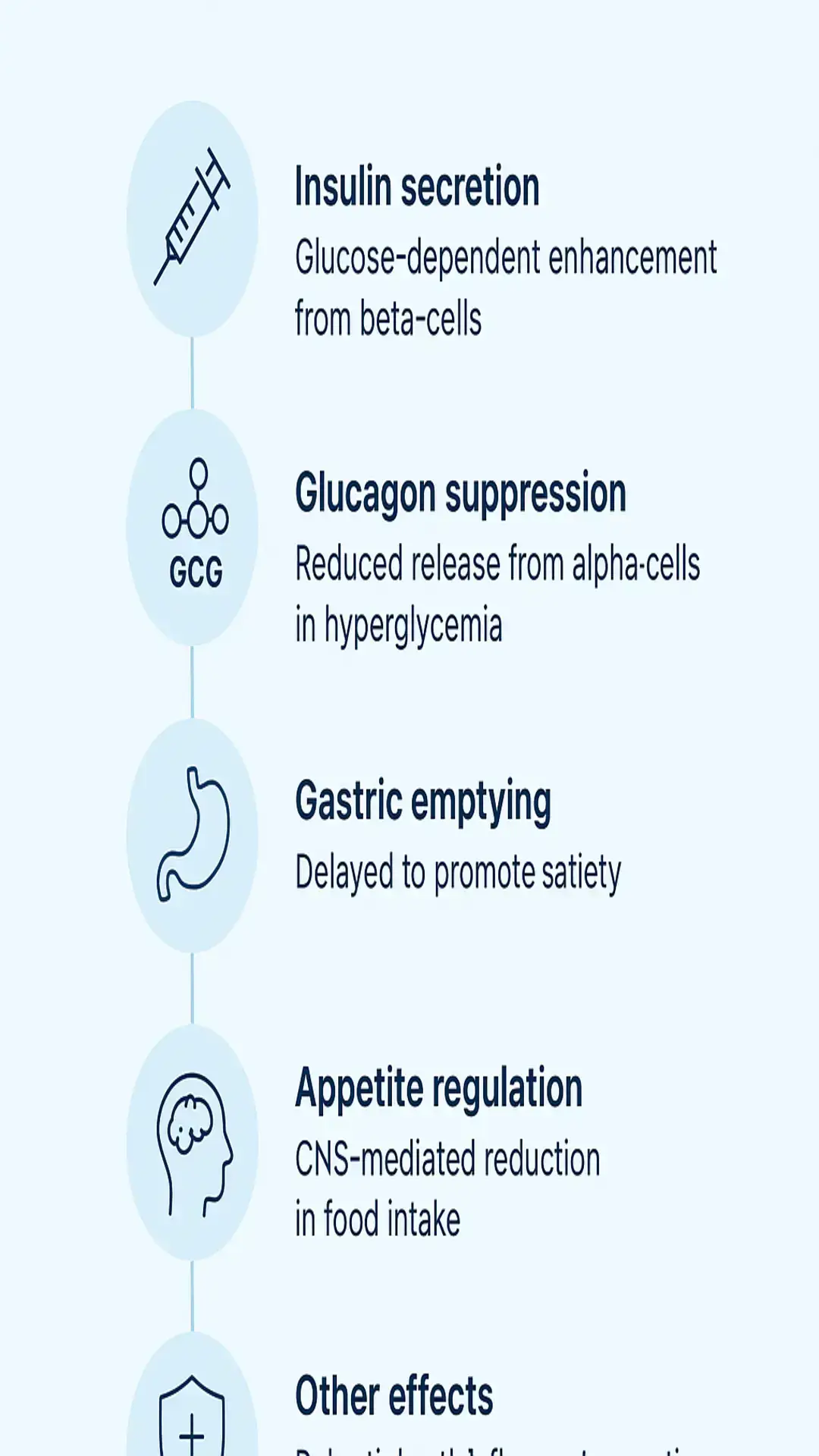
GLP-1RAs exert their effects by binding to GLP-1 receptors located on various tissues, including pancreatic beta-cells. This binding stimulates glucose-dependent insulin secretion, meaning insulin release is enhanced primarily when blood glucose levels are elevated.
They also suppress glucagon release from pancreatic alpha-cells specifically during periods of hyperglycemia, which helps reduce hepatic glucose production. Additionally, these agents slow gastric emptying, which can promote a feeling of satiety and help moderate postprandial glucose excursions. These statements have not been evaluated by the Food and Drug Administration. These products are not intended to diagnose, treat, cure, or prevent any disease.
Central nervous system effects are notable as well, with GLP-1 receptors in the brain contributing to appetite suppression and reduced food intake. Furthermore, GLP-1RAs demonstrate glucagonostatic effects during hyperglycemia and may support anti-inflammatory processes, though these are areas of ongoing research.
| Key Mechanisms | Description |
|---|---|
| Insulin secretion | Glucose-dependent enhancement from beta-cells |
| Glucagon suppression | Reduced release from alpha-cells in hyperglycemia |
| Gastric emptying | Delayed to promote satiety |
| Appetite regulation | CNS-mediated reduction in food intake |
| Other effects | Potential anti-inflammatory actions |
Therapeutic Applications
GLP-1RAs are FDA-approved for improving glycemic control in adults with T2DM, often alongside diet and exercise, and many users experience weight loss as a secondary effect. They are also indicated for chronic weight management in adults with obesity or overweight conditions accompanied by at least one weight-related comorbidity.
In patients with T2DM and established cardiovascular disease (CVD) or multiple risk factors, certain GLP-1RAs have shown reductions in cardiovascular events. Emerging research explores their roles in supporting liver health in non-alcoholic fatty liver disease, as well as potential benefits in heart failure and chronic kidney disease. These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
Clinical Evidence Supporting GLP-1RAs
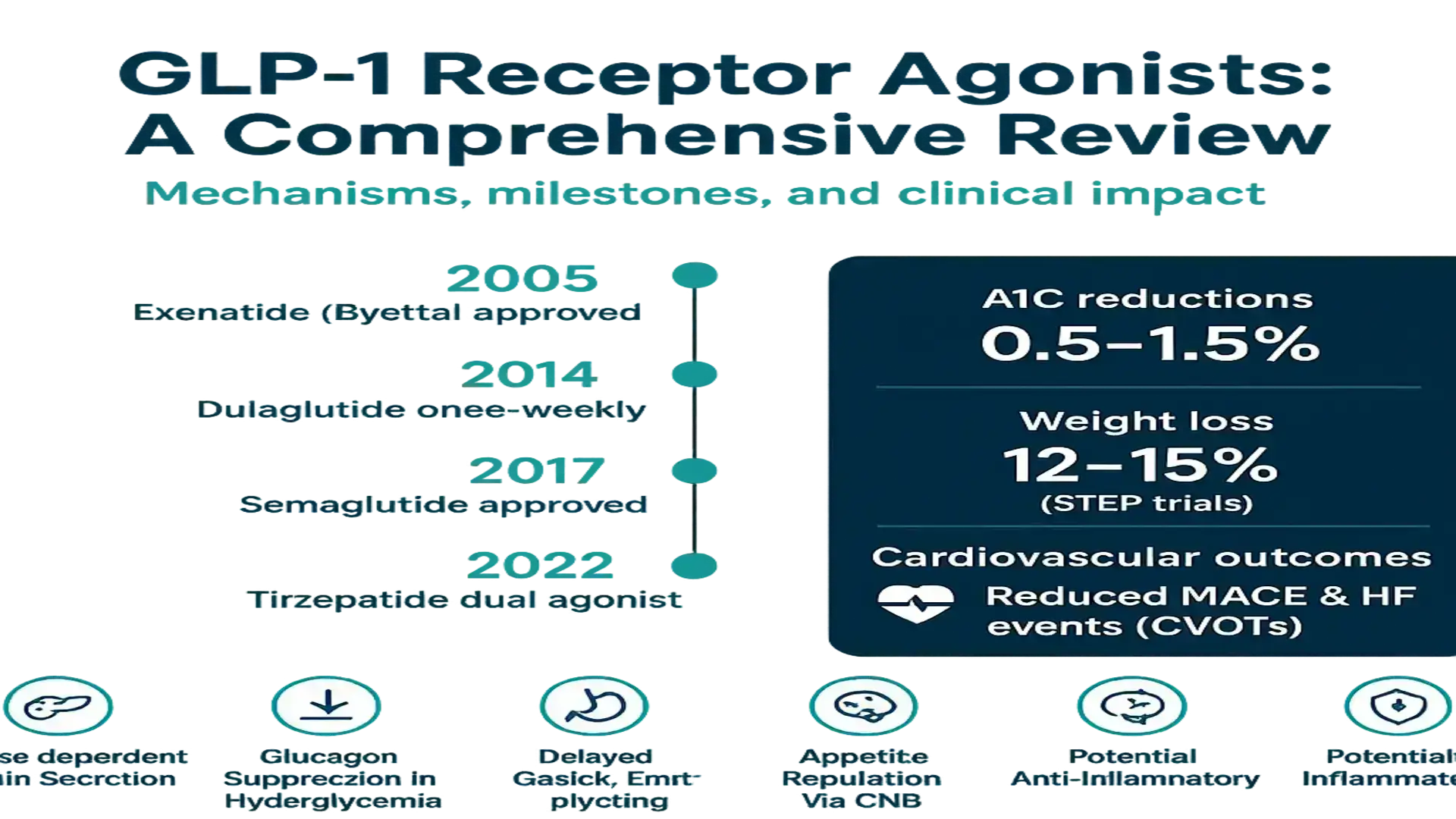
Numerous clinical trials and meta-analyses provide robust data on GLP-1RAs. Head-to-head studies indicate reductions in A1C levels ranging from 0.5% to 1.5% with agents like semaglutide and liraglutide. Network meta-analyses highlight their advantages over placebo or other antidiabetic medications in terms of HbA1c lowering, body weight reduction, and improvements in lipid profiles.
Cardiovascular outcome trials (CVOTs) have demonstrated reductions in major adverse cardiovascular events (MACE), heart failure hospitalizations, and mortality in high-risk T2DM populations. For weight management, trials such as the STEP program with semaglutide 2.4 mg showed average body weight reductions of 12-15% over 68 weeks in adults with obesity.
- Glycemic Control: Superior HbA1c reductions vs. comparators (e.g., Sun et al., BMJ 2024).
- Weight Loss: 12-15% reductions in obesity trials (e.g., STEP trials).
- CV Benefits: Lower MACE and HF events in CVOTs (e.g., Wang et al., 2024).
- Lipids: Improvements in cholesterol profiles per meta-analyses.
These findings are supported by systematic reviews and real-world evidence, affirming GLP-1RAs’ positions in treatment guidelines.
Challenges and Limitations
Despite their benefits, GLP-1RAs are associated with common gastrointestinal (GI) side effects, such as nausea, vomiting, diarrhea, and constipation, which often improve over time but can lead to discontinuation.
Safety concerns include potential risks of pancreatitis, gastroparesis, bowel obstruction, and biliary disorders compared to some other therapies. Weight loss maintenance requires ongoing use, with regain common upon discontinuation. Other barriers include high costs, the need for injections (though oral options are emerging), limited access, and potential antibody development with certain agents like exenatide. Contraindications exist for individuals with a history of pancreatitis or medullary thyroid carcinoma.
Monitoring strategies, dose titration, and patient education are essential to mitigate these issues.
Future Directions
The pipeline for GLP-1RAs is promising, with oral small-molecule agonists like orforglipron in development to eliminate injection needs and boost adherence. Dual and triple agonists, such as those combining GLP-1/GIP/glucagon receptor activation (e.g., tirzepatide), offer potential for greater weight loss and cardiometabolic improvements.
Research is expanding into non-diabetic populations, investigating roles in neurodegenerative conditions, addiction, and cognitive health. Ongoing trials assess outcomes in heart failure, kidney function, and long-term cancer risks.
Conclusion
GLP-1 receptor agonists stand out for their evidence-based contributions to glycemic control, weight management, and cardiovascular protection in appropriate populations with T2DM and obesity. Backed by clinical trials and meta-analyses, they often outperform placebo and select antidiabetics. While GI tolerability poses the main challenge, strategies for management exist. Innovations in formulations and indications suggest GLP-1 therapies will have an even broader impact moving forward. Consult healthcare providers for personalized advice. These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.
References
- Brikou D, et al. CNS Drugs. 2024;29(5). DOI:10.1017/S1092852924000123.
- Wang Y, et al. PubMed. 2024; PMID:39910752.
- Abd El Aziz M, et al. Ther Adv Chronic Dis. 2021;12:2040622321995797. PMC7953228.
- Tran K, et al. EClinicalMedicine. 2025;70:102595. PMC12303005.
- Sun F, et al. BMJ. 2024;384:e076410.
- Singh AK, et al. PubMed. 2024; PMID:39761578.
- Li X, et al. Front Endocrinol (Lausanne). 2024;15:11840199. PMC11840199.
- Nadkarni P, et al. Front Endocrinol (Lausanne). 2024;15:1431292.
- Awad K, et al. StatPearls. 2023. NBK551568.
- Zhang H, et al. Signal Transduct Target Ther. 2024;9(1):1931.
References
References
- Brikou D, et al. CNS Drugs. 2024;29(5). DOI:10.1017/S1092852924000123.
- Wang Y, et al. PubMed. 2024; PMID:39910752.
- Abd El Aziz M, et al. Ther Adv Chronic Dis. 2021;12:2040622321995797. PMC7953228.
- Tran K, et al. EClinicalMedicine. 2025;70:102595. PMC12303005.
- Sun F, et al. BMJ. 2024;384:e076410.
- Singh AK, et al. PubMed. 2024; PMID:39761578.
- Li X, et al. Front Endocrinol (Lausanne). 2024;15:11840199. PMC11840199.
- Nadkarni P, et al. Front Endocrinol (Lausanne). 2024;15:1431292.
- Awad K, et al. StatPearls. 2023. NBK551568.
- Zhang H, et al. Signal Transduct Target Ther. 2024;9(1):1931.