GLP-1 Receptor Agonists: A Comprehensive Review of Mechanisms and Clinical Insights
- By Isaac
GLP-1 Receptor Agonists: A Comprehensive Review of Mechanisms and Clinical Insights
GLP-1 receptor agonists (GLP-1 RAs) represent a significant class of medications designed to mimic the actions of the endogenous incretin hormone glucagon-like peptide-1 (GLP-1). These agents are primarily prescribed for glycemic control in adults with type 2 diabetes mellitus (T2DM) and for weight management in obesity (for certain agents). By promoting glucose-dependent insulin secretion, suppressing glucagon, delaying gastric emptying, and reducing appetite, GLP-1 RAs support improved blood sugar regulation and body weight reduction.
These statements have not been evaluated by the Food and Drug Administration. This information is for educational purposes and is not intended to diagnose, treat, cure, or prevent any disease.
This review provides an overview of GLP-1 RAs, including their background, mechanisms of action, clinical applications, evidence from key trials, potential limitations, and future developments, drawing from peer-reviewed studies.
Mechanisms of Action
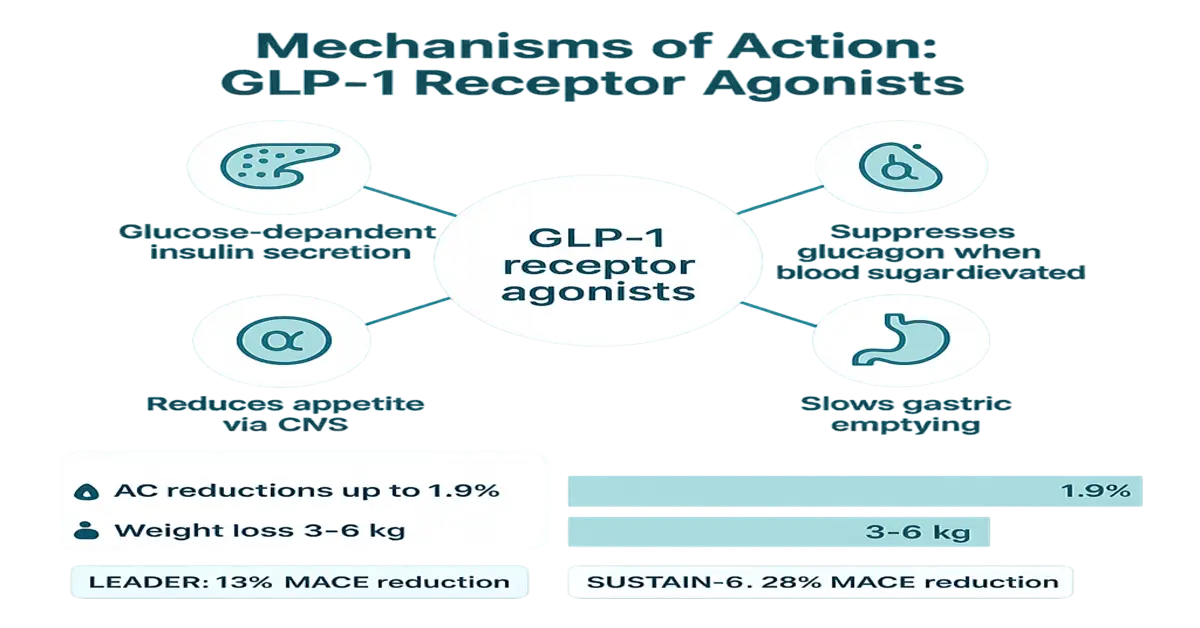
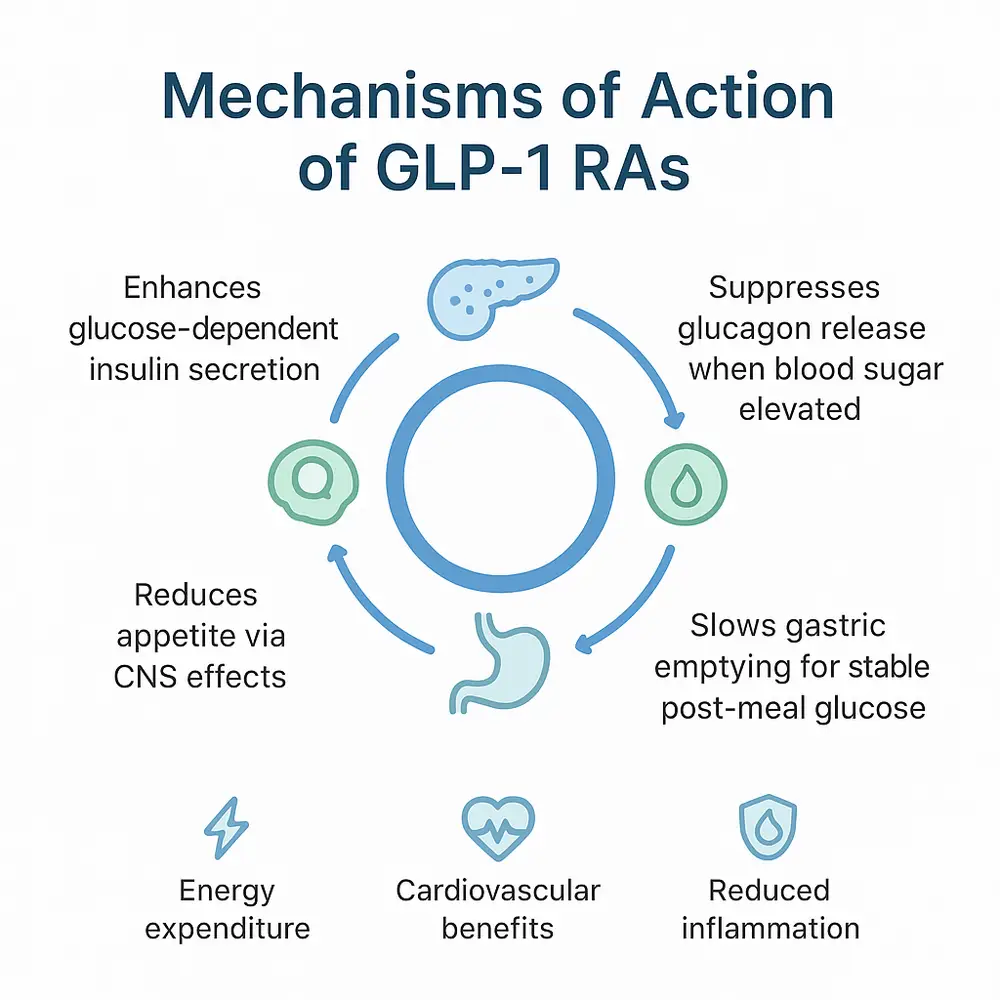
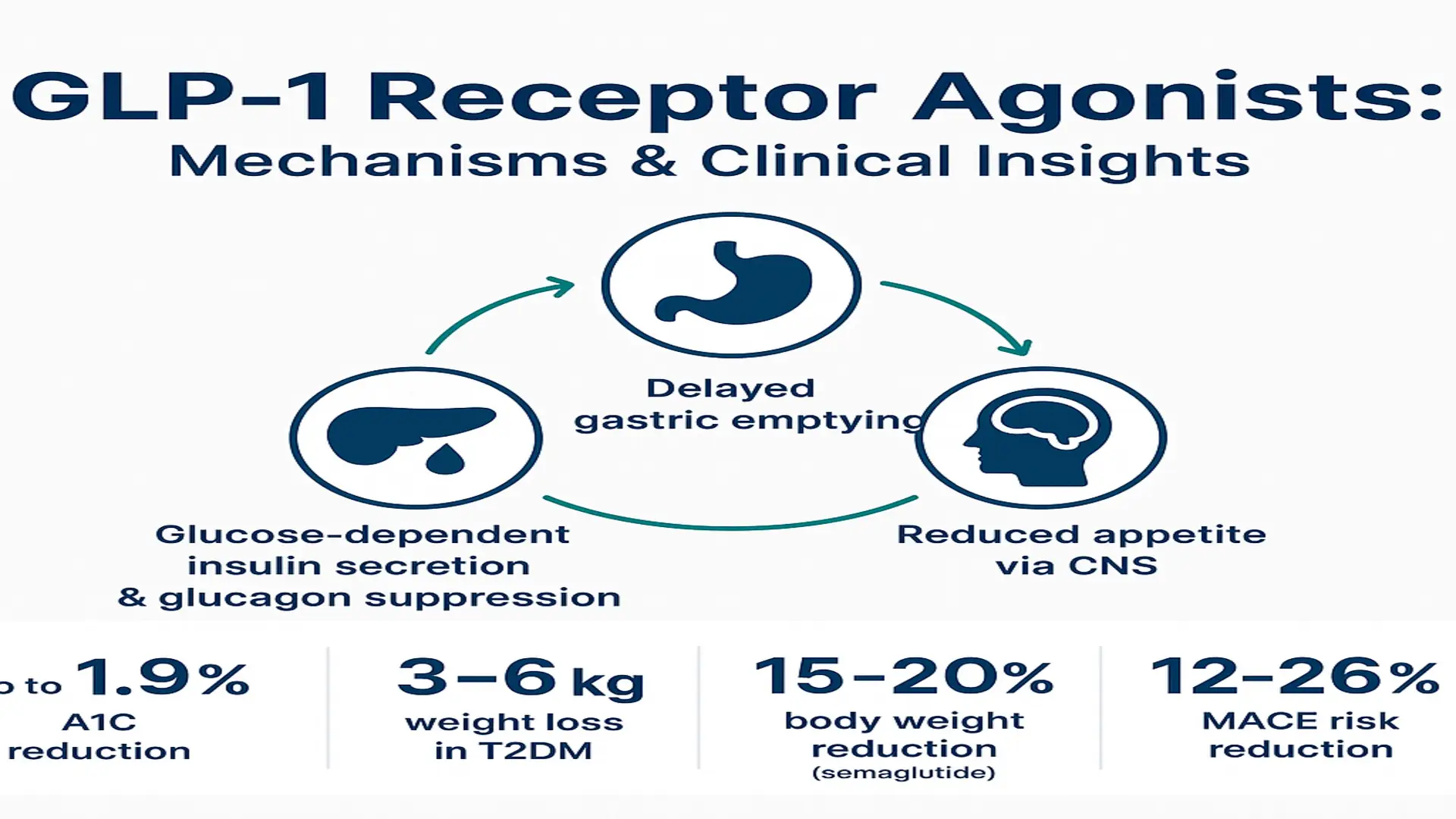
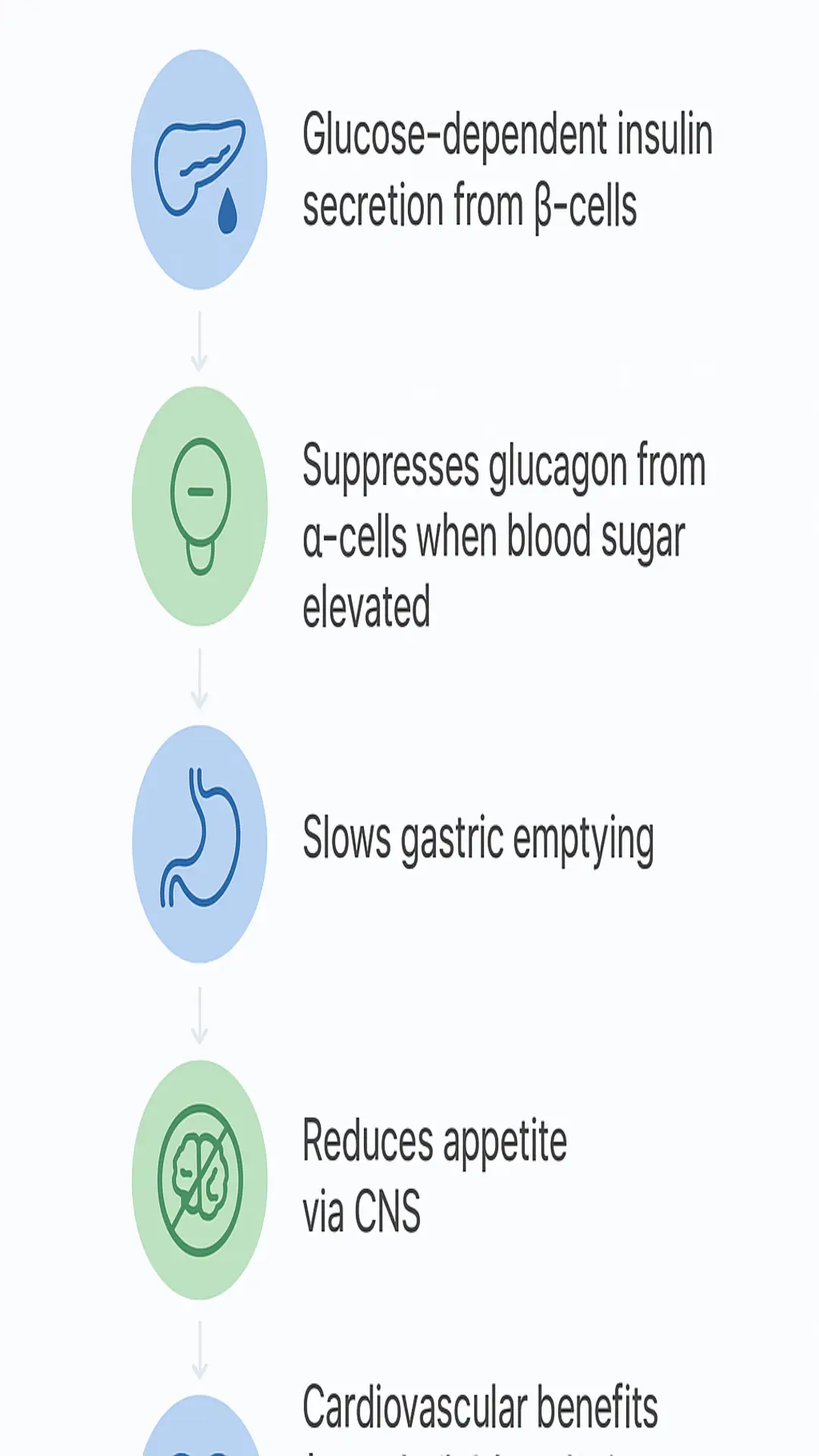
GLP-1 RAs work by binding to GLP-1 receptors located on pancreatic β-cells, which enhances insulin secretion in a glucose-dependent manner and suppresses glucagon release from α-cells specifically when blood sugar levels are elevated. This targeted action helps minimize the risk of hypoglycemia relative to some other glucose-lowering therapies. Additionally, these agonists slow gastric emptying, which contributes to more stable post-meal glucose levels.
Central nervous system effects are also prominent, as GLP-1 RAs influence hypothalamic pathways to reduce appetite and food intake. Preclinical models suggest further benefits, such as increased energy expenditure through brown fat activation and stimulation of the sympathetic nervous system. Cardiovascular effects may stem from improvements in endothelial function, reduced inflammation, and direct signaling that supports heart and vessel health.
These statements have not been evaluated by the Food and Drug Administration. This information is for educational purposes and is not intended to diagnose, treat, cure, or prevent any disease.
Therapeutic Applications
In clinical practice, GLP-1 RAs have been shown in clinical trials to support A1C reductions of up to 1.9% and average weight loss of 3-6 kg, either as monotherapy or in combination with other therapies for glycemic management in T2DM. For weight management in non-diabetic individuals with obesity, agents like semaglutide have demonstrated, in some clinical trials, 15-20% body weight reduction.
Certain GLP-1 RAs, such as liraglutide and semaglutide, carry indications for cardiovascular risk reduction in some T2DM patients with high risk, based on reductions in major adverse cardiovascular events. Emerging observational data points to potential roles in conditions like polycystic ovary syndrome (PCOS), non-alcoholic fatty liver disease (NAFLD), and substance use disorders, though further research is needed.
These statements have not been evaluated by the Food and Drug Administration. This information is for educational purposes and is not intended to diagnose, treat, cure, or prevent any disease.
Clinical Evidence Supporting GLP-1 RAs
Head-to-head trials indicate that GLP-1 RAs achieve A1C reductions of 0.5-1.8% and weight loss of 2-5 kg over 26-52 weeks, outperforming placebo. Meta-analyses reinforce these findings, showing consistent decreases in BMI, waist circumference, and overall body weight across diverse patient populations.
Major cardiovascular outcome trials, such as LEADER (for liraglutide) and SUSTAIN-6 (for semaglutide), report relative reductions of 12-26% in the risk of major adverse cardiovascular events. Long-term studies with high-dose semaglutide and dulaglutide demonstrate sustained support for glycemic control and weight management.
| Key Trial Examples | A1C Reduction | Weight Loss | Cardiovascular Benefit |
|---|---|---|---|
| Head-to-Head Trials (26-52 weeks) | 0.5-1.8% | 2-5 kg | N/A |
| LEADER (Liraglutide) | Variable | Variable | 13% MACE reduction |
| SUSTAIN-6 (Semaglutide) | Up to 1.8% | Up to 5 kg | 26% MACE reduction |
These statements have not been evaluated by the Food and Drug Administration. This information is for educational purposes and is not intended to diagnose, treat, cure, or prevent any disease.
Challenges and Limitations
While effective, GLP-1 RAs are associated with common gastrointestinal side effects, including nausea, vomiting, and diarrhea, which contribute to discontinuation rates of 5-10% and are often related to dosing. There is an increased risk of cholelithiasis (relative risk 1.46), and although pancreatitis has been investigated, it is not consistently linked. Cardiovascular harm has not been consistently observed in large trials.
Upon discontinuation, weight regain can occur, with meta-analyses indicating partial reversal of prior losses. Other barriers include high costs, the need for injections in many formulations, and occasional supply shortages, all of which can affect accessibility and adherence.
Future Directions
Advancements include oral formulations, such as oral semaglutide, and small-molecule agonists aimed at improving patient adherence by eliminating injections. Multi-agonist therapies, like GLP-1/GIP dual agonists (e.g., tirzepatide), have shown superior weight loss of up to 22% in phase 3 trials.
Ongoing research explores applications in neuroprotection, addiction treatment, and broader cardiovascular and kidney outcomes. Clinical guidelines stress the importance of combining GLP-1 RAs with lifestyle interventions, such as diet and exercise, for optimal, sustained results.
Conclusion
GLP-1 receptor agonists offer evidence-based support for glycemic control, weight management, and cardiovascular protection in appropriate patients with T2DM and obesity. Backed by clinical trials and meta-analyses, their benefits may outweigh gastrointestinal risks for many individuals. However, personalized approaches are essential to address side effects, costs, and adherence challenges. Emerging oral and multi-receptor options hold promise for wider accessibility and expanded uses in GLP-1-related therapies.
References
- Trujillo JM, et al. (2021). GLP-1 receptor agonists: an updated review of head-to-head clinical studies. Curr Diabetes Rep. 21(4):10.
- Filippatos TD, et al. (2014). Adverse Effects of GLP-1 Receptor Agonists. Rev Diabet Stud. 11(3-4):202-230.
- Wong HJ, et al. (2025). Efficacy of GLP-1 Receptor Agonists on Weight Loss, BMI, and Waist Circumference: A Systematic Review and Meta-Analysis. Cureus. 17(2):e39841.
- Müller TD, et al. (2019). Glucagon-like peptide 1 (GLP-1). Mol Metab. 30:72-130.
- Moore PW IV. (2023). GLP-1 Agonists for Weight Loss: Pharmacology and Clinical Implications. J Clin Pharmacol. 63 Suppl 1:S16-S27.
- Collins L, Costello RA. (2024). Glucagon-Like Peptide-1 Receptor Agonists. StatPearls [Internet].
- Drucker DJ. (2018). Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1. Cell Metab. 27(4):740-756.
- Liu QK, et al. (2024). Mechanisms of action and therapeutic applications of GLP-1/GIP receptor agonists in diabetes and obesity. Front Endocrinol (Lausanne). 15:1431292.
- Popoviciu MS, et al. (2023). Emerging Role of GLP-1 Agonists in Obesity: A Systematic Review of Randomized Controlled Trials. Int J Mol Sci. 24(14):11366.
- Ghusn W, et al. (2024). Weight loss outcomes, tolerability, side effects, and risks associated with GLP-1R agonist medications: a systematic review and network meta-analysis. Obes Rev. 25(10):e13824.
References
References
- Trujillo JM, et al. (2021). GLP-1 receptor agonists: an updated review of head-to-head clinical studies. Curr Diabetes Rep. 21(4):10.
- Filippatos TD, et al. (2014). Adverse Effects of GLP-1 Receptor Agonists. Rev Diabet Stud. 11(3-4):202-230.
- Wong HJ, et al. (2025). Efficacy of GLP-1 Receptor Agonists on Weight Loss, BMI, and Waist Circumference: A Systematic Review and Meta-Analysis. Cureus. 17(2):e39841.
- Müller TD, et al. (2019). Glucagon-like peptide 1 (GLP-1). Mol Metab. 30:72-130.
- Moore PW IV. (2023). GLP-1 Agonists for Weight Loss: Pharmacology and Clinical Implications. J Clin Pharmacol. 63 Suppl 1:S16-S27.
- Collins L, Costello RA. (2024). Glucagon-Like Peptide-1 Receptor Agonists. StatPearls [Internet].
- Drucker DJ. (2018). Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1. Cell Metab. 27(4):740-756.
- Liu QK, et al. (2024). Mechanisms of action and therapeutic applications of GLP-1/GIP receptor agonists in diabetes and obesity. Front Endocrinol (Lausanne). 15:1431292.
- Popoviciu MS, et al. (2023). Emerging Role of GLP-1 Agonists in Obesity: A Systematic Review of Randomized Controlled Trials. Int J Mol Sci. 24(14):11366.
- Ghusn W, et al. (2024). Weight loss outcomes, tolerability, side effects, and risks associated with GLP-1R agonist medications: a systematic review and network meta-analysis. Obes Rev. 25(10):e13824.