GLP1 Meds: Research on Mechanisms and Clinical Trial Findings
- By Isaac
GLP-1 receptor agonists (GLP-1RAs), known as GLP1 meds, are incretin mimetics.
They were originally developed for glycemic control in type 2 diabetes.
These GLP1 meds include semaglutide, liraglutide, and dulaglutide.
Research has expanded to obesity management and cardiovascular risk reduction.
This review synthesizes evidence from clinical trials, meta-analyses, and guidelines on efficacy, safety, and applications [1,2,3].
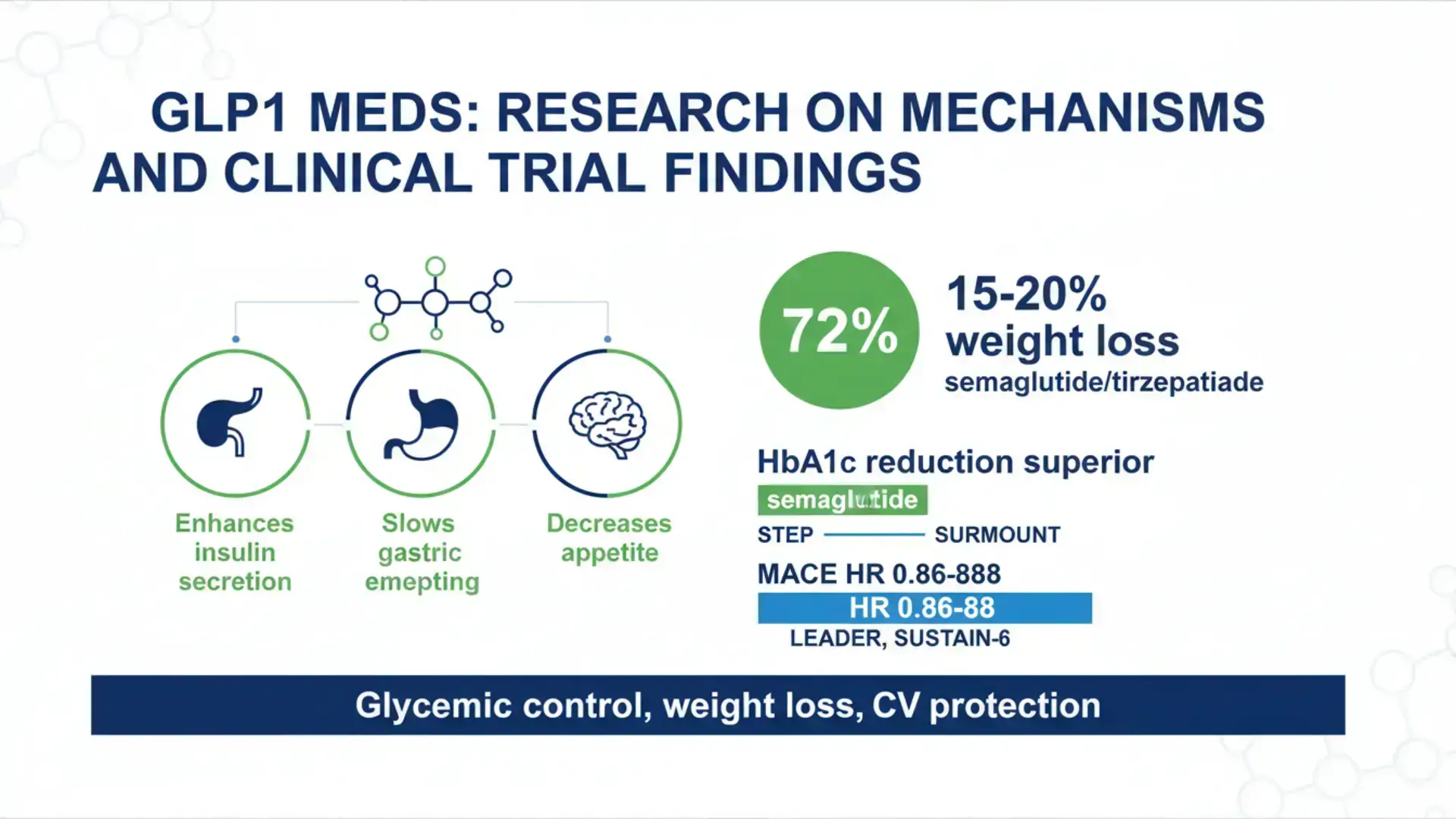
GLP1 meds bind GLP-1 receptors on pancreatic beta-cells. This enhances glucose-dependent insulin secretion.
They suppress glucagon release from alpha-cells.
This reduces hepatic glucose production.
GLP1 meds slow gastric emptying.
This promotes satiety and reduces postprandial glucose excursions.
They act centrally in the hypothalamus.
This decreases appetite and food intake.
They also improve endothelial function and reduce inflammation.
Dual/triple agonists (e.g., tirzepatide GLP-1/GIP) enhance weight loss.
They do this via additional receptor targeting [1,4,7].
Research on GLP1 meds has focused on type 2 diabetes for glycemic control.
This is when metformin is insufficient.
Studies have examined use in patients with cardiovascular disease.
Clinical trials have investigated chronic weight management in obesity/overweight with comorbidities (semaglutide, liraglutide).
Trials have assessed cardiovascular risk reduction in type 2 diabetes with established CVD or high risk.
Emerging research includes non-alcoholic steatohepatitis (NASH) and polycystic ovary syndrome (PCOS).
Potential neuroprotection for Parkinson’s has also been noted.
Studies have combined GLP1 meds with lifestyle interventions for effects on weight and metabolic outcomes [1,2,8].
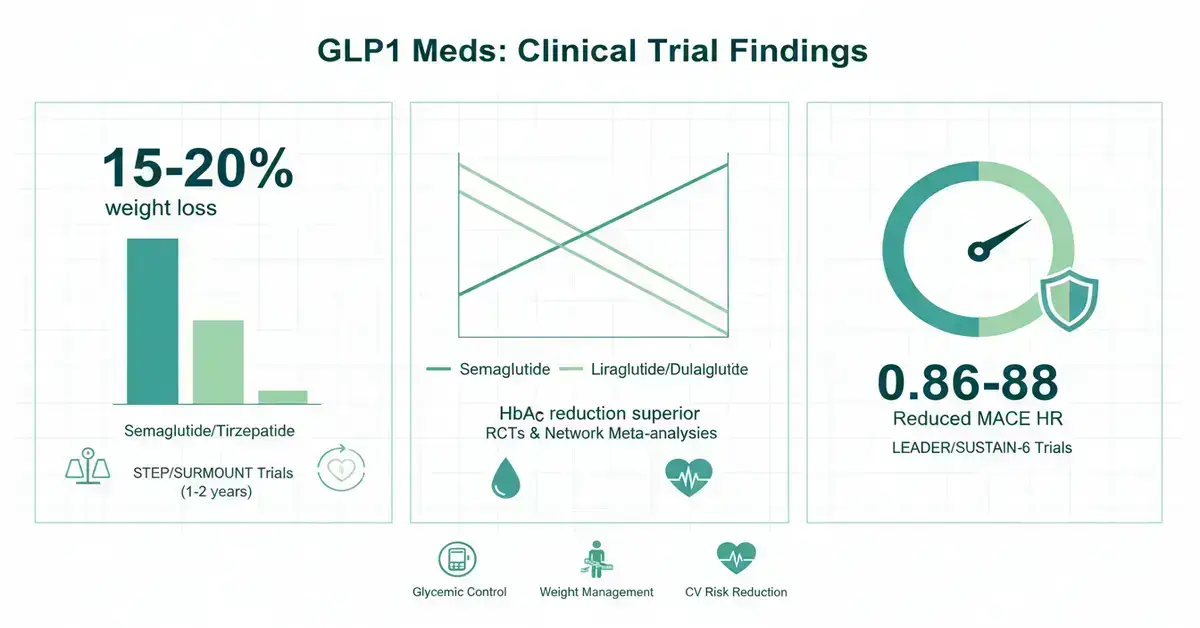
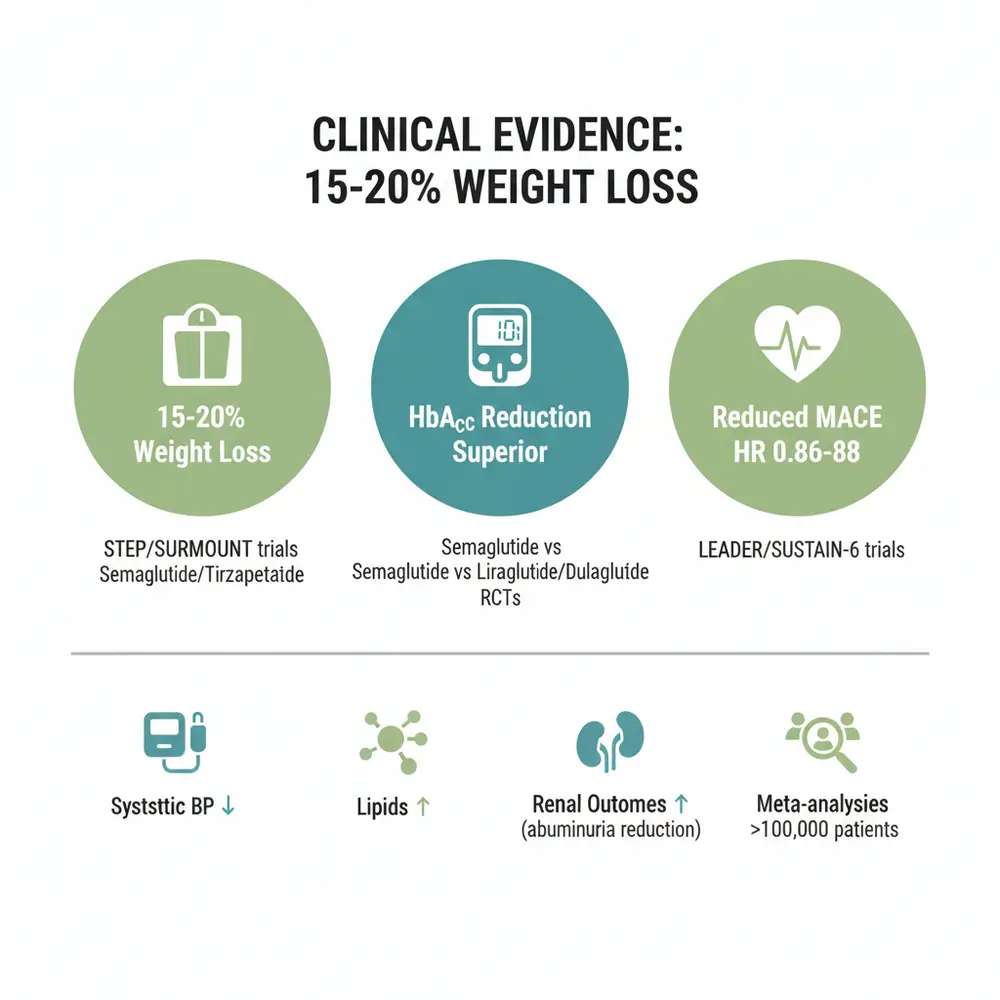
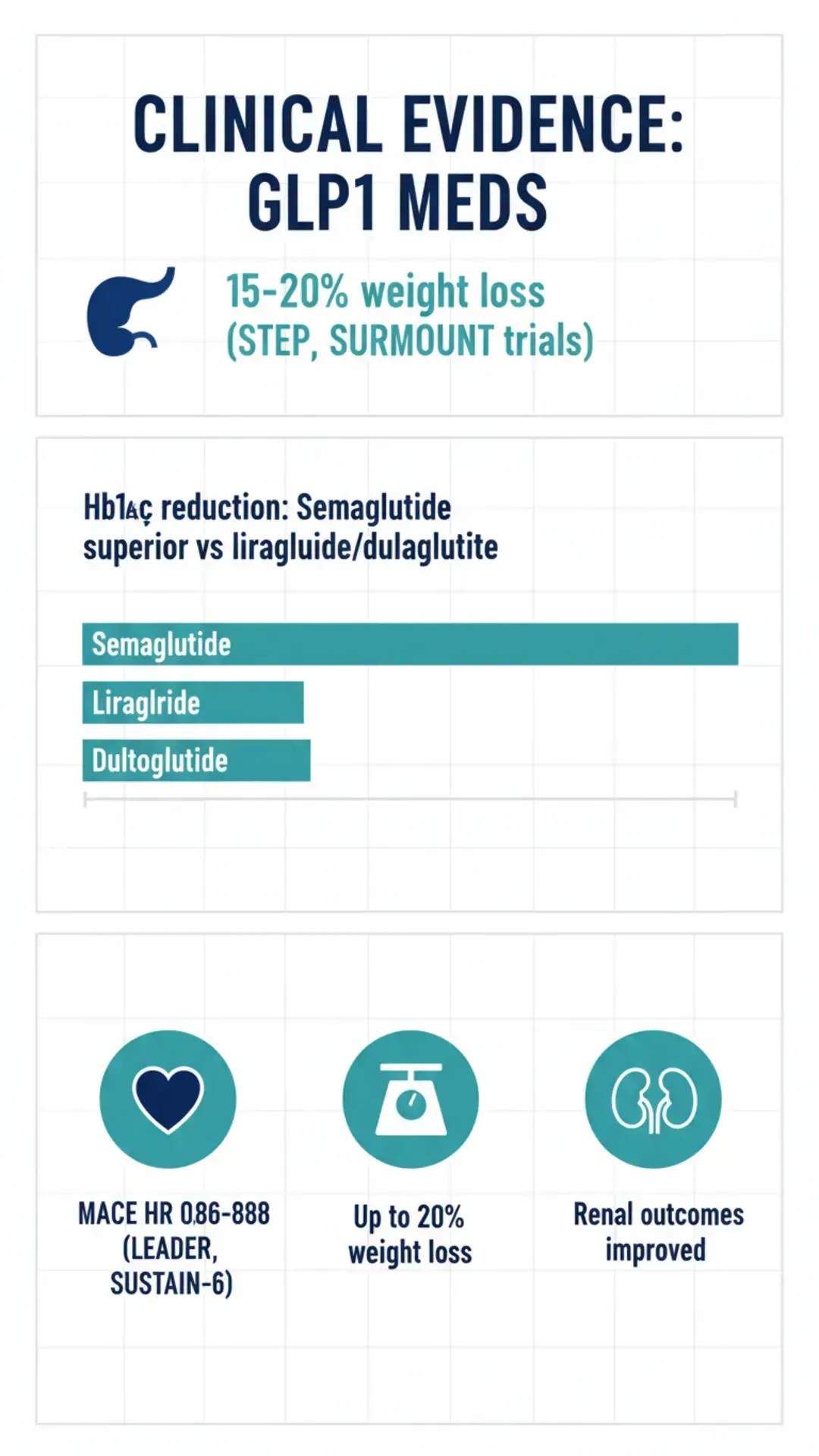
Meta-analyses show 15-20% weight loss with semaglutide/tirzepatide vs placebo.
This is over 1-2 years in obesity trials (STEP, SURMOUNT).
Superior HbA1c reduction with semaglutide vs liraglutide/dulaglutide.
Seen in head-to-head RCTs and network meta-analyses.
Cardiovascular outcome trials (LEADER, SUSTAIN-6) demonstrate reduced MACE (HR 0.86-0.88) with liraglutide/semaglutide.
Cochrane reviews confirm clinically meaningful weight loss with GLP1 meds vs placebo.
This is sustained during treatment.
Improvements in systolic BP, lipids, and renal outcomes (e.g., albuminuria reduction).
Across large RCTs (>100,000 patients) [3,5,9,10,11].
Common gastrointestinal adverse events include nausea (higher with semaglutide).
Also vomiting and diarrhea, leading to discontinuation.
Increased risk of gallbladder disorders with prolonged use and rapid weight loss.
Cholelithiasis RR 1.27, cholecystitis RR 1.36.
Weight regain after discontinuation: mean 9.7 kg with semaglutide/tirzepatide; 2.2 kg with liraglutide.
High cost, access issues, and need for subcutaneous injection (oral semaglutide available).
Limited long-term data beyond 2-3 years.
Industry-funded trials raise bias concerns [1,2,3,6].
Independent, long-term studies are needed for sustained weight management.
Non-industry funding is recommended (Cochrane/WHO).
Combination therapies (GLP-1 + exercise, dual/triple agonists) to preserve muscle mass.
This enhances adherence.
Expanded indications: neurodegenerative diseases (Alzheimer’s, Parkinson’s), addiction behaviors, type 1 diabetes adjunct.
Oral formulations, cost-effectiveness improvements, and equitable access strategies.
Ongoing trials for NASH resolution, heart failure, and broader CV/renal outcomes [1,2,3,4,8].
GLP1 meds provide robust evidence for glycemic control.
Clinical trials show substantial weight loss (up to 20%) and cardiorenal protection in type 2 diabetes and obesity.
Superior efficacy with semaglutide/tirzepatide per meta-analyses.
Chronic therapy is required to maintain effects.
Lifestyle integration optimizes outcomes.
Guidelines (ADA, EASD, WHO) discuss this class.
Access and long-term data gaps persist [1,2,3,8,10].
1. Liu Z, et al. (2025). The Clinical Application of GLP-1RAs and GLP-1/GIP Dual Agonists. *Front Med*. https://pmc.ncbi.nlm.nih.gov/articles/PMC12653004/
2. Moiz A, et al. (2025). The expanding role of GLP-1 receptor agonists. *Lancet eClinMed*. https://pmc.ncbi.nlm.nih.gov/articles/PMC12303005/
3. Cochrane Library. (2025). GLP-1 drugs effective for weight loss, but more independent studies needed. https://www.cochrane.org/about-us/news/glp-1-drugs-effective-weight-loss-more-independent-studies-needed
4. Xie Z, et al. (2024). Seven glucagon-like peptide-1 receptor agonists and polyagonists. PubMed PMID: 39305981. https://pubmed.ncbi.nlm.nih.gov/39305981/
5. Sattar N, et al. (2021). Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists. *Lancet Diabetes Endocrinol*. PubMed PMID: 34425083. https://pubmed.ncbi.nlm.nih.gov/34425083/
6. Silverii GA, et al. (2024). GLP-1 receptor agonists and the risk for cancer: A meta-analysis. PubMed PMID: 40437949. https://pubmed.ncbi.nlm.nih.gov/40437949/
7. Moiz A, et al. (2024). Mechanisms of GLP-1 Receptor Agonist-Induced Weight Loss. PubMed PMID: 39892489. https://pubmed.ncbi.nlm.nih.gov/39892489/
8. WHO. (2024). World Health Organization Guideline on GLP-1 Therapies for Obesity in Adults. *JAMA*. https://jamanetwork.com/journals/jama/fullarticle/2842199
9. Guo H, et al. (2025). GLP-1 agonists for weight reduction: Meta-analysis. PubMed. https://pmc.ncbi.nlm.nih.gov/articles/PMC11840199/
10. Karimi MA, et al. (2025). Comparative effectiveness of semaglutide versus other GLP-1RAs. PubMed. https://pmc.ncbi.nlm.nih.gov/articles/PMC12120964/
11. Derington CG, et al. (2025). Liraglutide vs Semaglutide vs Dulaglutide in Veterans. *JAMA Netw Open*. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2840010
References
1. Liu Z, et al. (2025). The Clinical Application of GLP-1RAs and GLP-1/GIP Dual Agonists. *Front Med*. https://pmc.ncbi.nlm.nih.gov/articles/PMC12653004/
2. Moiz A, et al. (2025). The expanding role of GLP-1 receptor agonists. *Lancet eClinMed*. https://pmc.ncbi.nlm.nih.gov/articles/PMC12303005/
3. Cochrane Library. (2025). GLP-1 drugs effective for weight loss, but more independent studies needed. https://www.cochrane.org/about-us/news/glp-1-drugs-effective-weight-loss-more-independent-studies-needed
4. Xie Z, et al. (2024). Seven glucagon-like peptide-1 receptor agonists and polyagonists. PubMed PMID: 39305981. https://pubmed.ncbi.nlm.nih.gov/39305981/
5. Sattar N, et al. (2021). Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists. *Lancet Diabetes Endocrinol*. PubMed PMID: 34425083. https://pubmed.ncbi.nlm.nih.gov/34425083/
6. Silverii GA, et al. (2024). GLP-1 receptor agonists and the risk for cancer: A meta-analysis. PubMed PMID: 40437949. https://pubmed.ncbi.nlm.nih.gov/40437949/
7. Moiz A, et al. (2024). Mechanisms of GLP-1 Receptor Agonist-Induced Weight Loss. PubMed PMID: 39892489. https://pubmed.ncbi.nlm.nih.gov/39892489/
8. WHO. (2024). World Health Organization Guideline on GLP-1 Therapies for Obesity in Adults. *JAMA*. https://jamanetwork.com/journals/jama/fullarticle/2842199
9. Guo H, et al. (2025). GLP-1 agonists for weight reduction: Meta-analysis. PubMed. https://pmc.ncbi.nlm.nih.gov/articles/PMC11840199/
10. Karimi MA, et al. (2025). Comparative effectiveness of semaglutide versus other GLP-1RAs. PubMed. https://pmc.ncbi.nlm.nih.gov/articles/PMC12120964/
11. Derington CG, et al. (2025). Liraglutide vs Semaglutide vs Dulaglutide in Veterans. *JAMA Netw Open*. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2840010