GLP-1 Medications: 11 Key Insights from Clinical Research
- By Isaac
GLP-1 Medications: 11 Key Insights from Clinical Research
Introduction
Glucagon-like peptide-1 receptor agonists (GLP-1RAs), commonly referred to as GLP-1 medications, represent a significant class of pharmaceuticals designed to mimic the action of the incretin hormone GLP-1. These medications are approved for use in the management of type 2 diabetes mellitus (T2DM) and obesity, offering benefits such as weight reduction, support for glycemic control, and cardiovascular risk reduction in certain populations [1][2].
Over the past decade, GLP-1 medications have reshaped approaches to obesity management and metabolic health, with clinical trials demonstrating substantial weight loss averaging 12-15% in some studies, alongside improvements in blood sugar levels and heart health markers [3][4]. This comprehensive review draws from peer-reviewed sources to explore the background, mechanisms of action, therapeutic applications, clinical evidence, challenges, and future directions of GLP-1 medications. Readers should consult healthcare professionals for personalized advice, as these are prescription medications requiring medical supervision.
These statements have not been evaluated by the Food and Drug Administration. This information is for educational purposes only and is not intended to diagnose, treat, cure, or prevent any disease.
Mechanisms of Action
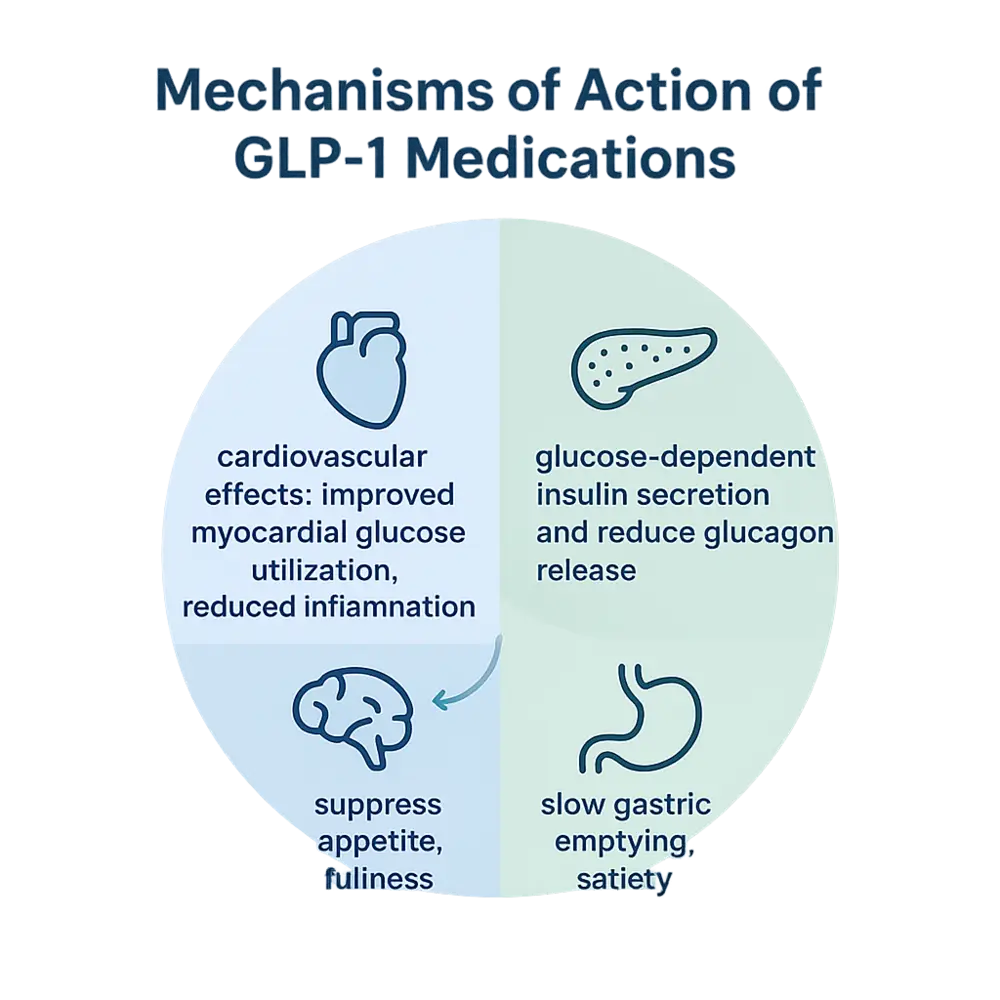
GLP-1 medications exert their effects by binding to GLP-1 receptors located on various tissues, including pancreatic β-cells, where they promote glucose-dependent insulin secretion and reduce glucagon release primarily during elevated blood glucose states [4][5]. This mechanism helps support balanced glucose levels without significantly increasing hypoglycemia risk.
In the gastrointestinal tract, these medications slow gastric emptying, which contributes to feelings of satiety and reduced calorie intake [3]. Central nervous system effects, particularly in the hypothalamus, further suppress appetite and promote a sense of fullness, influencing eating behaviors [1].
Beyond glycemic and appetite regulation, GLP-1 medications demonstrate cardiovascular effects, such as improved myocardial glucose utilization, reduced systemic inflammation, and beneficial hemodynamic changes like lowered blood pressure [2][6]. They also support lipid metabolism by promoting a shift toward fat oxidation, enhancing glycogen storage in the liver and muscles, and aiding in overall energy balance [5]. These multifaceted actions underscore their role in metabolic regulation, as evidenced in preclinical and clinical studies.
Therapeutic Applications
GLP-1 medications are primarily utilized as part of comprehensive management strategies for T2DM, often added to metformin or used as initial therapy in patients with established cardiovascular disease (CVD) or chronic kidney disease, aligning with American Diabetes Association (ADA) guidelines [6][7]. For weight management, agents like semaglutide (Wegovy®) and liraglutide (Saxenda®) are FDA-approved for adults with obesity or overweight with comorbidities, while tirzepatide (Zepbound®/Mounjaro®) is approved for similar indications in adults aged 18 and older [1][2].
In cardiovascular health, select GLP-1 medications, such as liraglutide and semaglutide, are indicated to reduce the risk of major adverse cardiovascular events (MACE), including heart attack, stroke, and cardiovascular death, in adults with T2DM and established CVD [4]. Pediatric approvals include liraglutide and semaglutide for adolescents aged 12 and older with obesity, and semaglutide for T2DM in those aged 10 and older [8].
These statements have not been evaluated by the Food and Drug Administration. This information is for educational purposes only and is not intended to diagnose, treat, cure, or prevent any disease. Always follow prescribing information and consult a healthcare provider.
Clinical Evidence
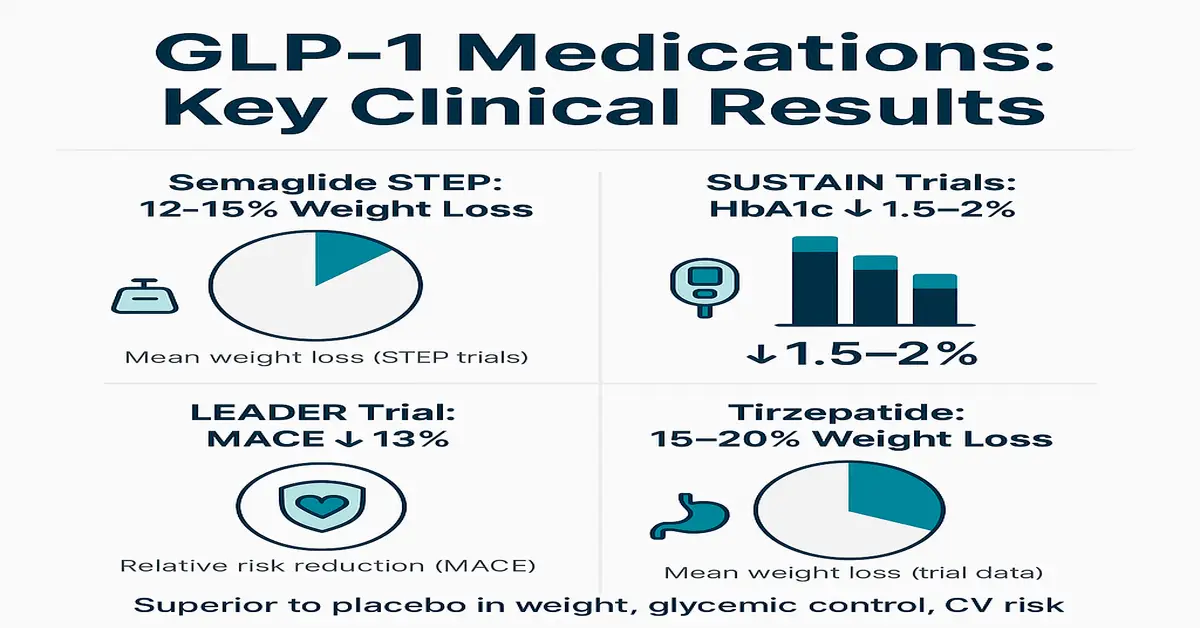
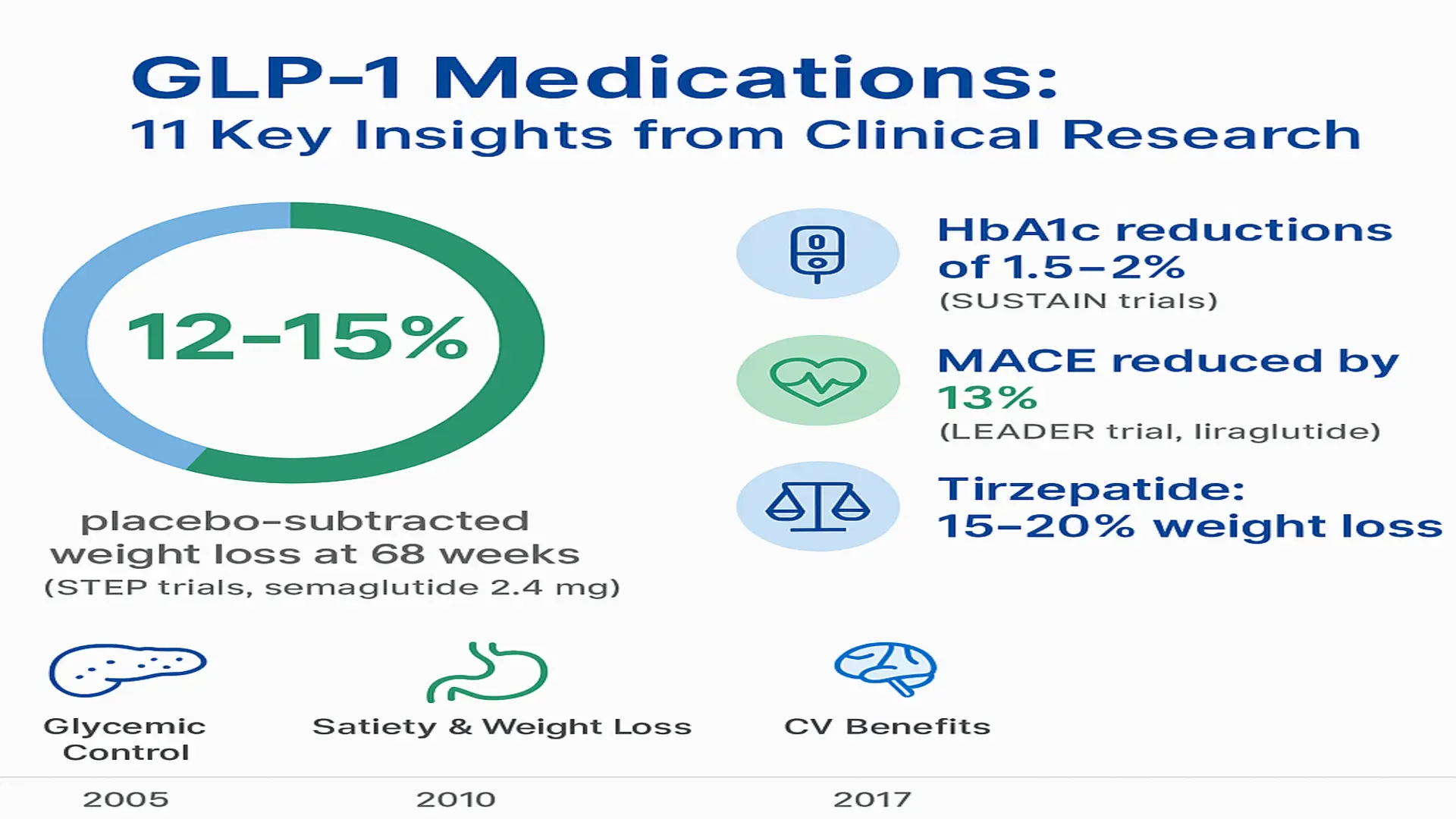
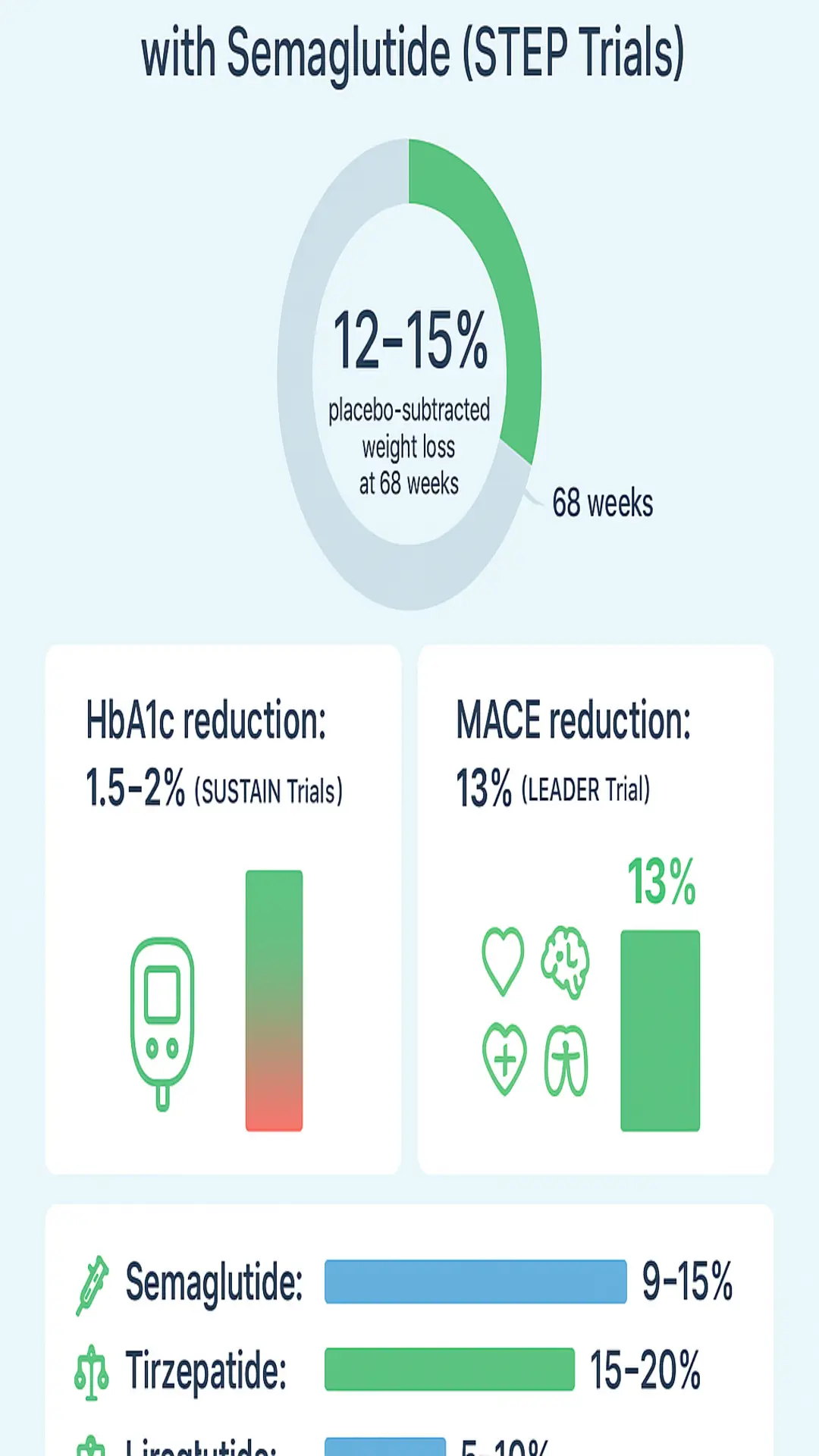
Extensive clinical trials provide robust data on GLP-1 medications. In the STEP program for obesity, semaglutide (2.4 mg weekly) achieved 12-15% placebo-subtracted weight loss at 68 weeks, with sustained glycemic improvements in T2DM trials like SUSTAIN, showing HbA1c reductions of 1.5-2% [1][10]. Liraglutide demonstrated cardiovascular benefits in the LEADER trial, reducing MACE by 13% in over 9,000 T2DM patients with high CVD risk, including lower rates of CV death, non-fatal myocardial infarction, and stroke [2].
Network meta-analyses of over 100 trials confirm GLP-1RAs outperform other antidiabetic classes in HbA1c reduction (up to 1%), weight loss (4-6 kg more than placebo), and lipid profile improvements, such as lowered triglycerides [6]. Cochrane reviews highlight clinically meaningful weight reductions with semaglutide (9-15%), tirzepatide (15-20%), and liraglutide (5-10%), maintained during treatment, alongside benefits for kidney function markers like albuminuria reduction [10]. Real-world studies reinforce these findings, though long-term data in non-T2DM populations remain emerging [9].
Challenges and Limitations
Despite their efficacy, GLP-1 medications are associated with gastrointestinal adverse effects, including nausea (up to 44%), vomiting (24%), diarrhea (30%), and abdominal pain (20%), which are often transient and dose-dependent but contribute to 5-10% discontinuation rates [8]. Meta-analyses report significant weight regain—up to 2/3 of lost weight—within one year of discontinuation, emphasizing the need for lifestyle integration [11].
Current challenges include global drug shortages, particularly for semaglutide, and risks with compounded versions lacking FDA approval, which have led to dosing errors, contamination, and severe adverse events like hospitalizations [7]. Emerging safety signals include potential associations with psychiatric events (e.g., mood changes), ocular conditions like non-arteritic anterior ischemic optic neuropathy (NAION), and reductions in lean body mass alongside fat loss; however, causality requires further investigation [8]. Long-term safety data in broader populations, including non-diabetics, are limited, with ongoing surveillance needed [9].
Future Directions
The pipeline for GLP-1 medications includes oral small-molecule GLP-1RAs like orforglipron, potentially improving adherence by eliminating injections and reducing GI tolerability issues [9]. Research is expanding into additional areas, such as chronic kidney disease, substance use disorders, neurodegenerative conditions like Alzheimer’s, and even asthma, based on pleiotropic effects observed in trials [5][9].
Priorities include independent long-term studies on safety profiles, strategies for weight maintenance after stopping therapy, and optimal combination regimens with other agents [10][11]. Addressing barriers like high costs (often $1,000+/month), access disparities, and equity will rely on real-world evidence, payer policies, and generic development amid surging prescriptions exceeding 15 million annually in the U.S. [1][7].
Conclusion
GLP-1 medications offer evidence-based support for weight management, glycemic control, and cardiovascular protection in approved populations with T2DM and obesity. Backed by large-scale trials like STEP, LEADER, and meta-analyses from sources such as Cochrane and BMJ, they demonstrate superior outcomes compared to many alternatives, with effects sustained during ongoing use [6][10].
However, gastrointestinal side effects, weight regain upon discontinuation, and other limitations highlight the importance of individualized prescribing, patient education, and lifestyle support [11]. As research advances formulations and indications, GLP-1 medications hold promise for broader metabolic health strategies, though continued monitoring and accessibility improvements are essential.
References
- Current Perspectives on GLP-1 Agonists in Contemporary Clinical …
- The expanding role of GLP-1 receptor agonists: a narrative review of …
- Mechanisms of action and therapeutic applications of GLP-1 and …
- Glucagon-Like Peptide-1 Receptor Agonists – StatPearls – NCBI – NIH
- Glucagon-like peptide-1 receptor: mechanisms and advances in …
- Comparative effectiveness of GLP-1 receptor agonists on glycaemic …
- The American Diabetes Association Announces Statement on …
- Exploring the Side Effects of GLP-1 Receptor Agonist: To Ensure Its …
- Emerging Frontiers in GLP-1 Therapeutics – MDPI
- GLP-1 drugs effective for weight loss, but more independent studies …
- Discontinuing glucagon-like peptide-1 receptor agonists and body …
References
References
- Current Perspectives on GLP-1 Agonists in Contemporary Clinical …
- The expanding role of GLP-1 receptor agonists: a narrative review of …
- Mechanisms of action and therapeutic applications of GLP-1 and …
- Glucagon-Like Peptide-1 Receptor Agonists – StatPearls – NCBI – NIH
- Glucagon-like peptide-1 receptor: mechanisms and advances in …
- Comparative effectiveness of GLP-1 receptor agonists on glycaemic …
- The American Diabetes Association Announces Statement on …
- Exploring the Side Effects of GLP-1 Receptor Agonist: To Ensure Its …
- Emerging Frontiers in GLP-1 Therapeutics – MDPI
- GLP-1 drugs effective for weight loss, but more independent studies …
- Discontinuing glucagon-like peptide-1 receptor agonists and body …