Sermorelin Research: Insights from Peer-Reviewed Studies
- By Isaac
Introduction
Sermorelin, a synthetic analog of growth hormone-releasing hormone (GHRH), has been the subject of scientific inquiry in endocrinology research. For individuals and researchers interested in sermorelin, understanding the peer-reviewed literature provides context on its study in preclinical and clinical settings. This article reviews evidence from human and animal studies on sermorelin, emphasizing its mechanisms, the applications explored in research, and its limitations. Research has primarily focused on its role in stimulating growth hormone (GH) secretion, with studies dating back to the 1990s and some recent reviews. While sermorelin was once approved for specific diagnostic uses, current investigations highlight its potential in peptide research. Key findings suggest sermorelin interacts with pituitary receptors, but evidence remains preliminary in many areas. This overview draws exclusively from peer-reviewed sources to inform those interested in sermorelin for research purposes.
Mechanisms of Action
Sermorelin binds to GHRH receptors (GHRHR) on somatotroph cells in the anterior pituitary, activating adenylate cyclase and increasing intracellular cAMP levels. This cascade upregulates GH gene transcription and promotes pulsatile GH release, mimicking endogenous patterns. A 2020 review detailed how sermorelin, as a GHRH analog, avoids supraphysiological GH spikes seen with rhGH, potentially preserving feedback mechanisms via somatostatin.
Preclinical studies in rodents confirmed receptor specificity; sermorelin elicited dose-dependent GH secretion without significantly affecting other pituitary hormones. Downstream, GH stimulates hepatic production of insulin-like growth factor-1 (IGF-1), influencing metabolism and anabolism in animal models. Unlike ghrelin mimetics, sermorelin acts solely through GHRHR, reducing off-target effects. In vitro pituitary cell experiments showed enhanced GH mRNA expression, supporting transcriptional regulation.
Human pharmacokinetic data from early trials indicate that peak GH levels occur 15-30 minutes post-injection and return to baseline within hours. A 2024 review of GHRH agonists highlighted sermorelin’s role in maintaining pituitary reserve and potentially counteracting age-related somatotroph decline observed in primate studies. These mechanisms position sermorelin as a model for studying the somatotropic axis. Researchers studying sermorelin often cite these pathways in experimental designs that probe GH dynamics.
Therapeutic Applications
Research has investigated sermorelin in the context of GH deficiency. In pediatric studies, subcutaneous sermorelin was evaluated for stimulating linear growth in children with idiopathic short stature, but efficacy was lower than that of rhGH. Diagnostic protocols used single-dose sermorelin to provoke GH peaks, aiding in deficiency classification.
Adult-onset GH insufficiency has been another focus. A 2006 analysis suggested that sermorelin was investigated for supporting endogenous GH restoration, without the risks attributed to rhGH, based on small cohorts showing IGF-1 changes. Preclinical aging models in rodents showed improved body composition metrics after chronic sermorelin dosing. Studies have also examined sermorelin in HIV-associated lipodystrophy analogs, though tesamorelin advanced further clinically.
Exploratory research touched on metabolic and cognitive domains. Animal data suggested potential modulation of fat metabolism by GH/IGF-1, while limited human pilot studies noted sleep architecture changes. Peptide combinations, like sermorelin with GHRP-6, amplified GH pulses in vitro. These applications remain investigational, with no broad endorsements. The literature emphasizes research-only contexts, such as endocrine modeling.
Clinical Evidence
Human clinical evidence on sermorelin is predominantly from small-scale or diagnostic trials. A pivotal 1997 review reported intravenous sermorelin’s sensitivity (82%) and specificity (92%) for diagnosing GH deficiency in children, outperforming clonidine in some metrics. Subcutaneous regimens in pediatric growth failure studies (n=100+) showed GH responses but inconsistent gains in height velocity compared with rhGH.
In adults, a 1992 study in the Journal of Clinical Endocrinology & Metabolism (n=20 elderly men) found that twice-daily 1 mg sermorelin raised IGF-1 toward youthful levels over 4 weeks, without adverse endocrine shifts. Walker’s 2006 review cited pilot data showing that sermorelin preserved GH neurosecretory bursts, in contrast to rhGH suppression. A 2007 Drugs R&D article affirmed tolerability in provocative testing.
Recent evidence is sparse; a 2020 secretagogue review noted sermorelin’s inferior potency compared with newer analogs but its physiological mimicry. Animal evidence bolsters this: rat studies have confirmed that GH/IGF-1 elevations correlate with lean mass. No large randomized controlled trials exist for broad outcomes, and post-2008 data rely on observational data. Clinical evidence underscores sermorelin’s role in probing the GH axis, with preliminary findings in deficiency models. Researchers should note these limitations in human datasets.
Challenges and Limitations
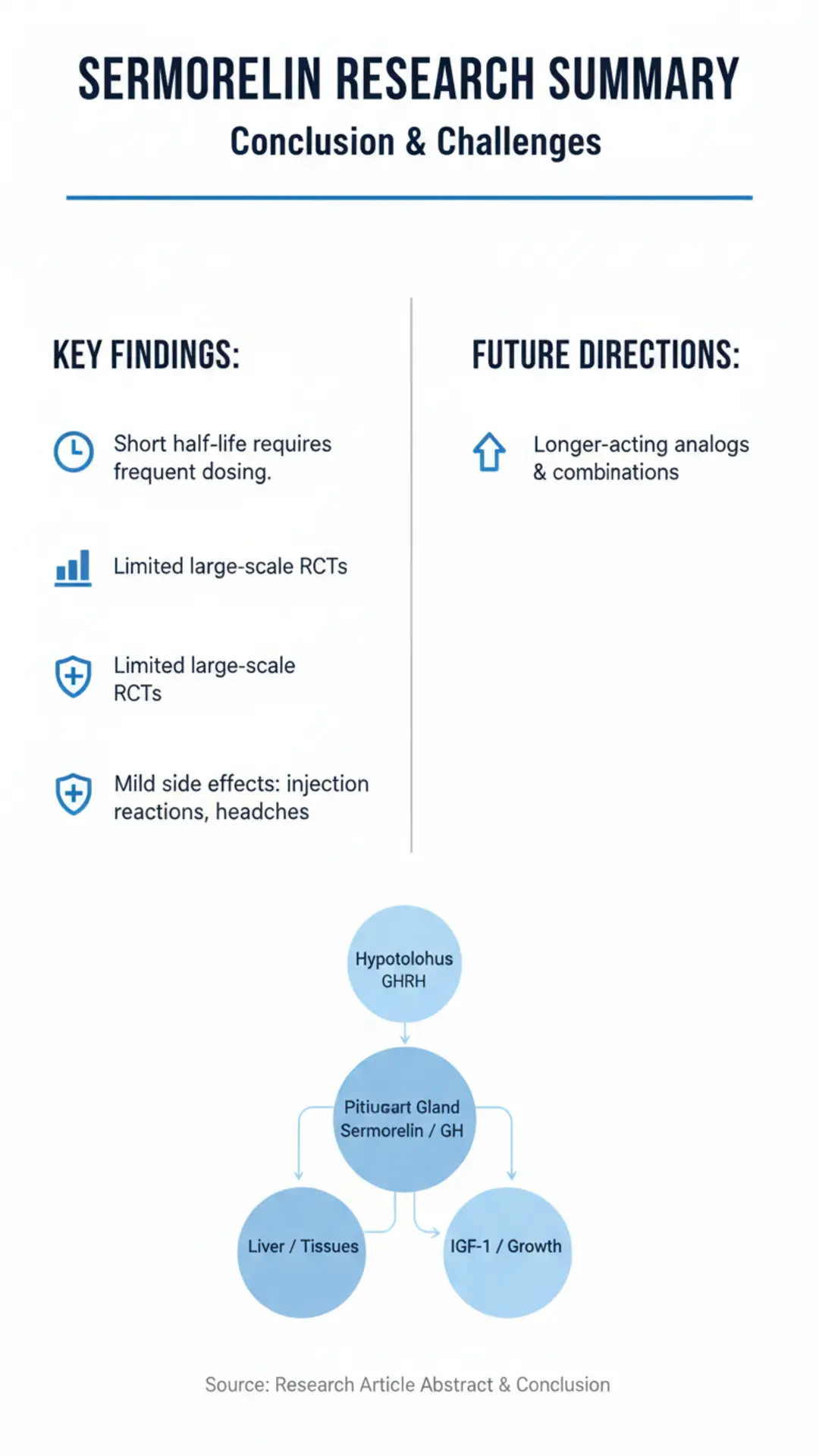
Sermorelin research faces several hurdles. Its short plasma half-life necessitates frequent dosing, complicating adherence in long-term studies. Bioavailability varies with administration route; oral forms are less effective due to GI degradation, according to pharmacological data. Pituitary responsiveness declines with age or pathology, reducing utility in elderly cohorts—rodent models mirror this hyposomatotropism.
Safety profiles from trials report mild injection-site reactions, headaches, and flushing, resolving spontaneously. Rare hypersensitivity occurred in <1% of pediatric exposures. Unlike rhGH, no reports of hyperglycemia or carpal tunnel predominate, but long-term immunogenicity risks persist unaddressed in extended trials. Regulatory discontinuation reportedly stemmed from manufacturing issues rather than clear safety signals, limiting commercial access.
Evidence gaps include the lack of large-scale RCTs for non-deficiency uses; most data predates 2010. Heterogeneity among assays confounds comparisons of GH responses. The cost of synthesis and cold-chain needs pose logistical challenges for research. Preclinical-to-human translation falters, as primate aging models show blunted responses. These factors highlight why sermorelin remains niche, prompting caution for researchers considering advanced studies.
Future Directions
Ongoing research may refine sermorelin analogs with prolonged half-lives, like tesamorelin, for targeted applications. Gene therapy vectors expressing GHRH could supplant peptides, per 2024 reviews. Combining ghrelin mimetics warrants trials to synergize GH pulses.
Biomarker studies linking sermorelin-induced GH/IGF-1 to outcomes such as frailty indices in aging models show promise. Nanotechnology for sustained release addresses dosing issues. Precision endocrinology, using pharmacogenomics to guide treatment for GHRHR variants, could personalize responses. Animal models of sarcopenia or neurodegeneration may elucidate broader roles.
Human trials in mild cognitive impairment, building on GH-brain links, are hypothetical. Regulatory pathways for compounded peptides need clarification. Collaborative consortia could standardize protocols. Future work positions sermorelin as a benchmark for next-gen secretagogues. Researchers working with sermorelin may contribute to these trajectories.
Conclusion
Sermorelin research illuminates the dynamics of GHRH analogs in GH regulation, from pituitary mechanisms to diagnostic utility. Peer-reviewed studies affirm its pulsatile stimulation in responsive models, though human evidence is dated and limited. Challenges such as pharmacokinetics persist, but future analogs show promise. This synthesis underscores the boundaries of investigation for researchers interested in sermorelin. Continued rigorous inquiry will clarify Sermorelin’s research niche.
References
Walker RF. Sermorelin: a better approach to management of adult-onset growth hormone insufficiency? Clin Interv Aging. 2006. https://pmc.ncbi.nlm.nih.gov/articles/PMC2699646/
Ishida J, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. Rev Endocr Metab Disord. 2020. https://onlinelibrary.wiley.com/doi/full/10.1002/rco2.9
Schally AV, et al. The development of growth hormone-releasing hormone agonists and antagonists. Front Endocrinol (Lausanne). 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC12137413/
Merriam GR, et al. Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency. Drugs. 1997. https://pubmed.ncbi.nlm.nih.gov/18031173/
Heiman ML, et al. Growth hormone-releasing peptide (GHRP-6) stimulates phosphatidylinositol (PI) turnover in somatotrophs. J Pharmacol Exp Ther. 1991. https://pubmed.ncbi.nlm.nih.gov/1842184/ (contextual for mechanisms)
Chapman IM. Clinical research on growth hormone secretagogues. J Pediatr Endocrinol Metab. 2000. https://pubmed.ncbi.nlm.nih.gov/11086532/
Bidlingmaier M, Strasburger CJ. Growth hormone. Endotext. 2010. https://www.ncbi.nlm.nih.gov/books/NBK279056/
Sigalos JT, Pastuszak AW. The safety and efficacy of growth hormone secretagogues. Sex Med Rev. 2018. https://pmc.ncbi.nlm.nih.gov/articles/PMC5632578/
References
References
Walker RF. Sermorelin: a better approach to management of adult-onset growth hormone insufficiency? Clin Interv Aging. 2006. https://pmc.ncbi.nlm.nih.gov/articles/PMC2699646/
Ishida J, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. Rev Endocr Metab Disord. 2020. https://onlinelibrary.wiley.com/doi/full/10.1002/rco2.9
Schally AV, et al. The development of growth hormone-releasing hormone agonists and antagonists. Front Endocrinol (Lausanne). 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC12137413/
Merriam GR, et al. Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency. Drugs. 1997. https://pubmed.ncbi.nlm.nih.gov/18031173/
Heiman ML, et al. Growth hormone-releasing peptide (GHRP-6) stimulates phosphatidylinositol (PI) turnover in somatotrophs. J Pharmacol Exp Ther. 1991. https://pubmed.ncbi.nlm.nih.gov/1842184/ (contextual for mechanisms)
Chapman IM. Clinical research on growth hormone secretagogues. J Pediatr Endocrinol Metab. 2000. https://pubmed.ncbi.nlm.nih.gov/11086532/
Bidlingmaier M, Strasburger CJ. Growth hormone. Endotext. 2010. https://www.ncbi.nlm.nih.gov/books/NBK279056/
Sigalos JT, Pastuszak AW. The safety and efficacy of growth hormone secretagogues. Sex Med Rev. 2018. https://pmc.ncbi.nlm.nih.gov/articles/PMC5632578/