GLP-1 Drugs: 12-20% Weight Loss in Clinical Studies – A Comprehensive Review
- By Isaac
GLP-1 Drugs: 12-20% Weight Loss in Clinical Studies – A Comprehensive Review
This information is for educational purposes only and is not intended to diagnose, treat, cure, or prevent any disease. Consult a qualified healthcare professional before starting or changing any medication or treatment plan.

Background
The foundation of GLP-1 drugs lies in the incretin hormone GLP-1, secreted by intestinal L-cells in response to nutrient intake. This hormone helps regulate post-meal glucose levels but has a very short half-life due to rapid breakdown by the enzyme dipeptidyl peptidase-4 (DPP-4). To address this limitation, GLP-1 receptor agonists were engineered as longer-acting analogs.
Early developments included short-acting formulations such as exenatide, administered twice daily and originally approved for use in type 2 diabetes mellitus (T2DM) management. Over time, the class evolved to include long-acting options such as weekly semaglutide, improving patient convenience. Innovations have extended to dual and multi-agonists, exemplified by tirzepatide, which targets both GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptors.
Regulatory bodies such as the FDA and EMA have approved specific GLP-1 agents for glycemic control in T2DM, for chronic weight management in defined populations with obesity (typically BMI ≥30 or ≥27 with weight-related conditions), and for reducing cardiovascular risk in certain high-risk patients. This progression reflects ongoing research into their multifaceted roles in metabolic health.
Mechanisms of Action
GLP-1 drugs bind to GLP-1 receptors on pancreatic β-cells, supporting glucose-dependent insulin secretion and helping suppress glucagon release in a glucose-dependent manner. These actions contribute to more balanced glucose levels without excessive insulin release in normoglycemic states.
Additional mechanisms include slowing gastric emptying, which can promote earlier satiety and reduce caloric intake, supporting body weight management. Central nervous system effects further enhance satiety signaling. Cardiovascular benefits observed in some studies may be related to improved myocardial glucose utilization, reductions in inflammatory markers, and effects on endothelial function.
Dual agonists such as tirzepatide include GIP receptor activation, which may augment insulin secretion and influence fat metabolism, providing a complementary profile to pure GLP-1 effects. These mechanisms collectively underpin the class’s observed effects in metabolic and cardiovascular research.
This content is educational and is not a substitute for professional medical advice.
Therapeutic Applications
In clinical practice, GLP-1 drugs are commonly used alongside lifestyle interventions and other glucose-lowering therapies (for example metformin) to help support HbA1c targets, with clinical trials typically reporting HbA1c reductions in the range of approximately 0.5–2.0% depending on baseline values and agent/dose, often accompanied by body weight decreases. For weight management, some GLP-1 receptor agonists are approved for chronic use in adults with obesity; clinical trials in selected non-diabetic populations have reported average body weight reductions in the range of about 12–15% over prolonged treatment periods.
Specific approvals exist for cardiovascular risk reduction in people with T2DM and established cardiovascular disease or multiple risk factors, as seen in trials of agents such as semaglutide and liraglutide. Emerging data from subgroup and exploratory analyses suggest possible roles in areas such as heart failure and chronic kidney disease, but definitive conclusions require additional research.
These applications highlight how GLP-1 drugs are being used to address interconnected metabolic factors within regulated, medical frameworks and under clinician supervision.
This content is educational and is not a substitute for professional medical advice.
Clinical Evidence
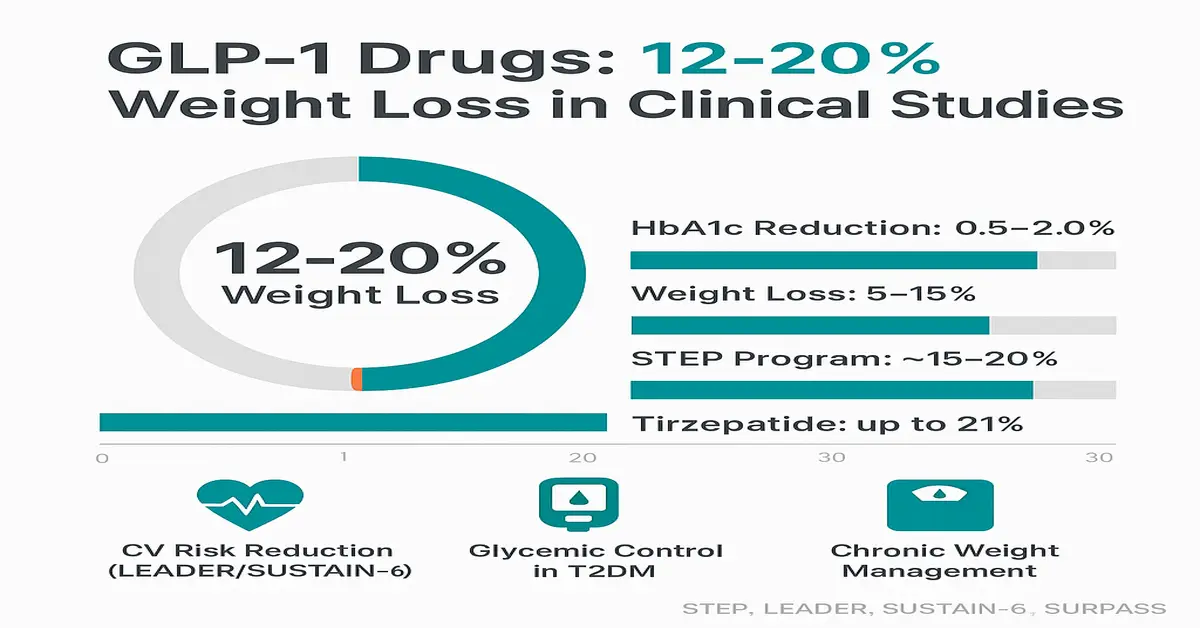
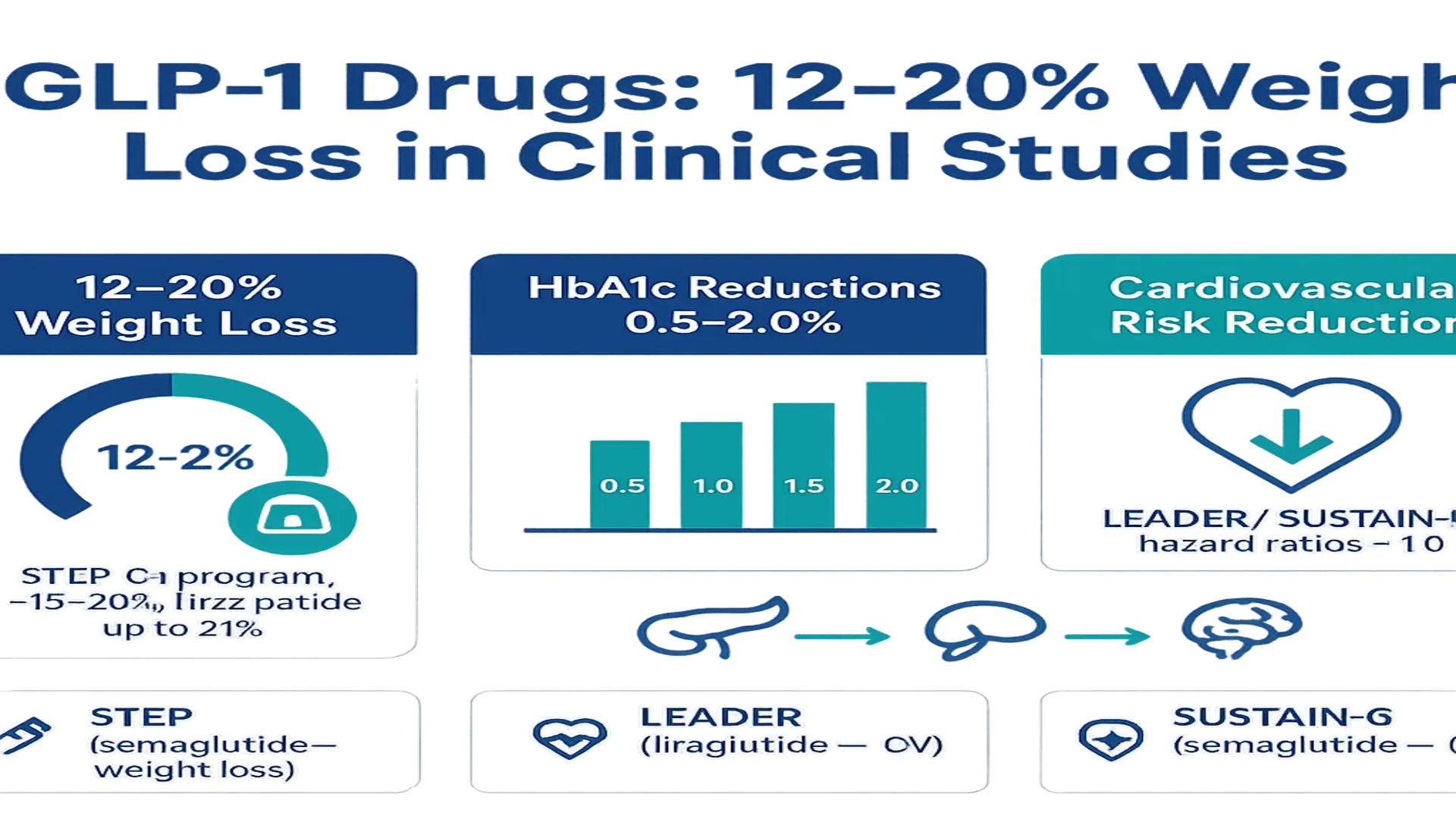
Meta-analyses and randomized controlled trials (RCTs) support the effects of GLP-1 drugs. Meta-analytic summaries report average HbA1c reductions in the approximate range of 0.5–1.5% and body weight decreases commonly reported between about 5–15%, while some cardiovascular outcome trials have found relative reductions in major adverse cardiovascular events (MACE) in selected high-risk T2DM populations compared with placebo or standard care.
The STEP program evaluated semaglutide 2.4 mg for weight management, demonstrating mean weight losses in the range of ~15–20% over 68 weeks in trial participants with obesity, and some head-to-head comparisons have suggested greater weight reductions with higher-efficacy agents compared with older GLP-1RAs. Landmark cardiovascular outcome trials such as LEADER (liraglutide) and SUSTAIN-6 (semaglutide) reported hazard ratios for MACE below 1.0 in high-risk T2DM cohorts, indicating relative risk reductions in those trial settings.
Network meta-analyses and head-to-head comparisons have positioned tirzepatide among the more efficacious agents for weight loss and glycemic lowering in clinical trials, with trial-reported weight reductions up to approximately 21% in selected study populations. These findings reflect results from controlled studies and may not predict individual outcomes in routine practice.
- Key trials: STEP (semaglutide for weight), LEADER/SUSTAIN-6 (cardiovascular outcomes), SURPASS (tirzepatide).
- Consistent findings in trials: weight loss, HbA1c lowering, and in some cases cardiovascular event risk reduction.
Challenges and Limitations
GLP-1 drugs commonly cause gastrointestinal adverse effects such as nausea, vomiting, and diarrhea; reported incidence varies by agent and dose, and may affect a substantial proportion of users, particularly during dose escalation. Discontinuation rates in trials vary. Rare but reported concerns include pancreatitis and gallbladder-related problems; rodent data suggested a theoretical risk of thyroid C-cell tumors with some agents, but human relevance appears limited and remains an area of ongoing monitoring and research.
Access and affordability remain major barriers for many patients due to high cost and supply issues in some markets. Compounded or unregulated products have prompted safety alerts from regulators because of potential inconsistencies. Other observations from trial data and observational studies include partial loss of lean mass in some individuals during weight loss, weight regain after discontinuation, and limited long-term safety and durability data beyond several years.
These issues are typically addressed through shared decision-making, careful monitoring, gradual dose titration, and supportive strategies in clinical practice.
Conclusion
Clinical studies have shown that GLP-1 receptor agonists can support glycemic control in people with T2DM, produce clinically meaningful weight loss in many trial participants (with reported ranges commonly cited between about 10–20% in certain studies), and, for some agents, reduce cardiovascular events in selected high-risk populations. Meta-analyses and major randomized trials such as STEP, LEADER, and SUSTAIN-6 provide evidence of these effects in controlled settings, though individual responses and tolerability vary.
Persistent challenges — including gastrointestinal side effects, cost, access, and questions about long-term durability — emphasize the need for individualized treatment decisions made with qualified healthcare professionals. Ongoing innovation in formulations and multi-receptor agents may expand therapeutic options, but extended studies are required to further define safety, durability, and personalized use.
References
- The expanding scope of GLP-1 receptor agonists: Six uses beyond …
- Current Perspectives on GLP-1 Agonists in Contemporary Clinical …
- Exploring the Side Effects of GLP-1 Receptor Agonist: To Ensure Its …
- The expanding role of GLP-1 receptor agonists: a narrative review of …
- Glucagon‐like peptide‐1 receptor agonist treatment reduces body …
- Glucagon-Like Peptide-1 Receptor Agonists – StatPearls – NCBI – NIH
- Mechanisms of action and therapeutic applications of GLP-1 and …
- Efficacy of GLP-1 Receptor Agonists on Weight Loss, BMI, and Waist …
- Comparative effectiveness of GLP-1 receptor agonists on glycaemic …
- WHO Guideline on GLP-1 Therapies for Obesity in Adults

References
References
- The expanding scope of GLP-1 receptor agonists: Six uses beyond …
- Current Perspectives on GLP-1 Agonists in Contemporary Clinical …
- Exploring the Side Effects of GLP-1 Receptor Agonist: To Ensure Its …
- The expanding role of GLP-1 receptor agonists: a narrative review of …
- Glucagon‐like peptide‐1 receptor agonist treatment reduces body …
- Glucagon-Like Peptide-1 Receptor Agonists – StatPearls – NCBI – NIH
- Mechanisms of action and therapeutic applications of GLP-1 and …
- Efficacy of GLP-1 Receptor Agonists on Weight Loss, BMI, and Waist …
- Comparative effectiveness of GLP-1 receptor agonists on glycaemic …
- WHO Guideline on GLP-1 Therapies for Obesity in Adults