GLP-1 Receptor Agonist Medicines: 10 Key Insights from Recent Research
- By Isaac
GLP-1 Receptor Agonist Medicines: 10 Key Insights from Recent Research
Introduction
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs), also known as GLP-1 receptor agonist medicines, are a class of incretin mimetics designed to activate GLP-1 receptors. These medications have been studied extensively for their roles in supporting glycemic control, weight management, cardiovascular health, and kidney function. Research highlights their potential in addressing metabolic challenges associated with type 2 diabetes and obesity. This review article explores the mechanisms, applications, clinical evidence, challenges, and future directions of GLP-1 receptor agonist medicines, drawing from recent peer-reviewed studies to provide an educational overview for readers interested in metabolic research.
These statements have not been evaluated by the Food and Drug Administration. This information is for educational purposes only and is not intended to diagnose, treat, cure, or prevent any disease.
Mechanisms of Action
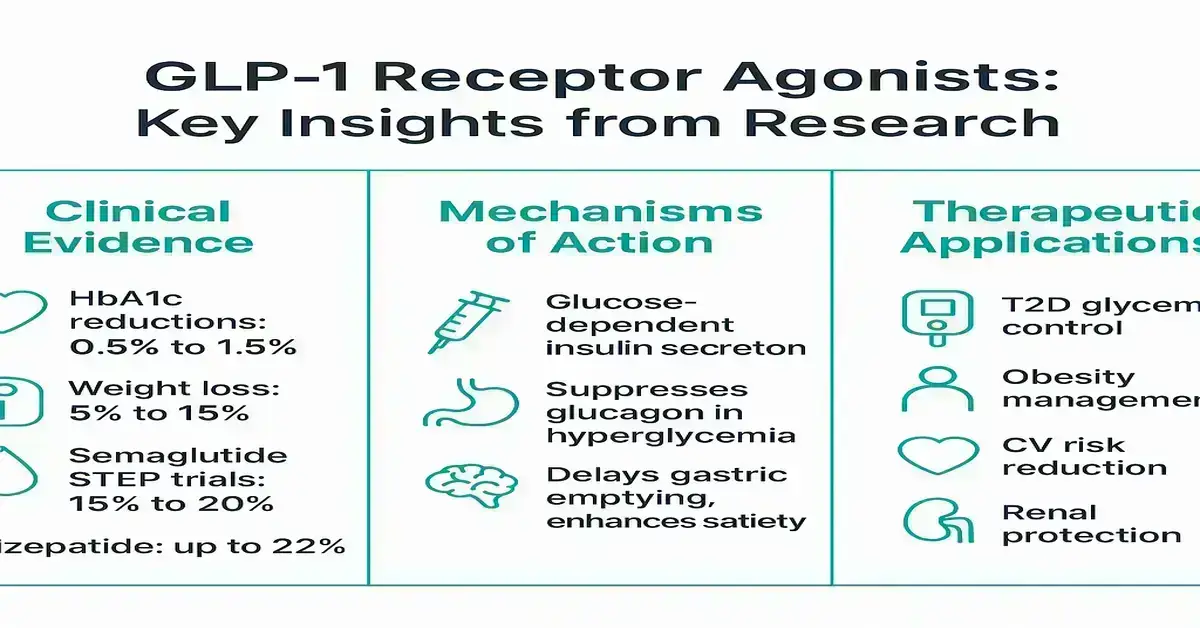
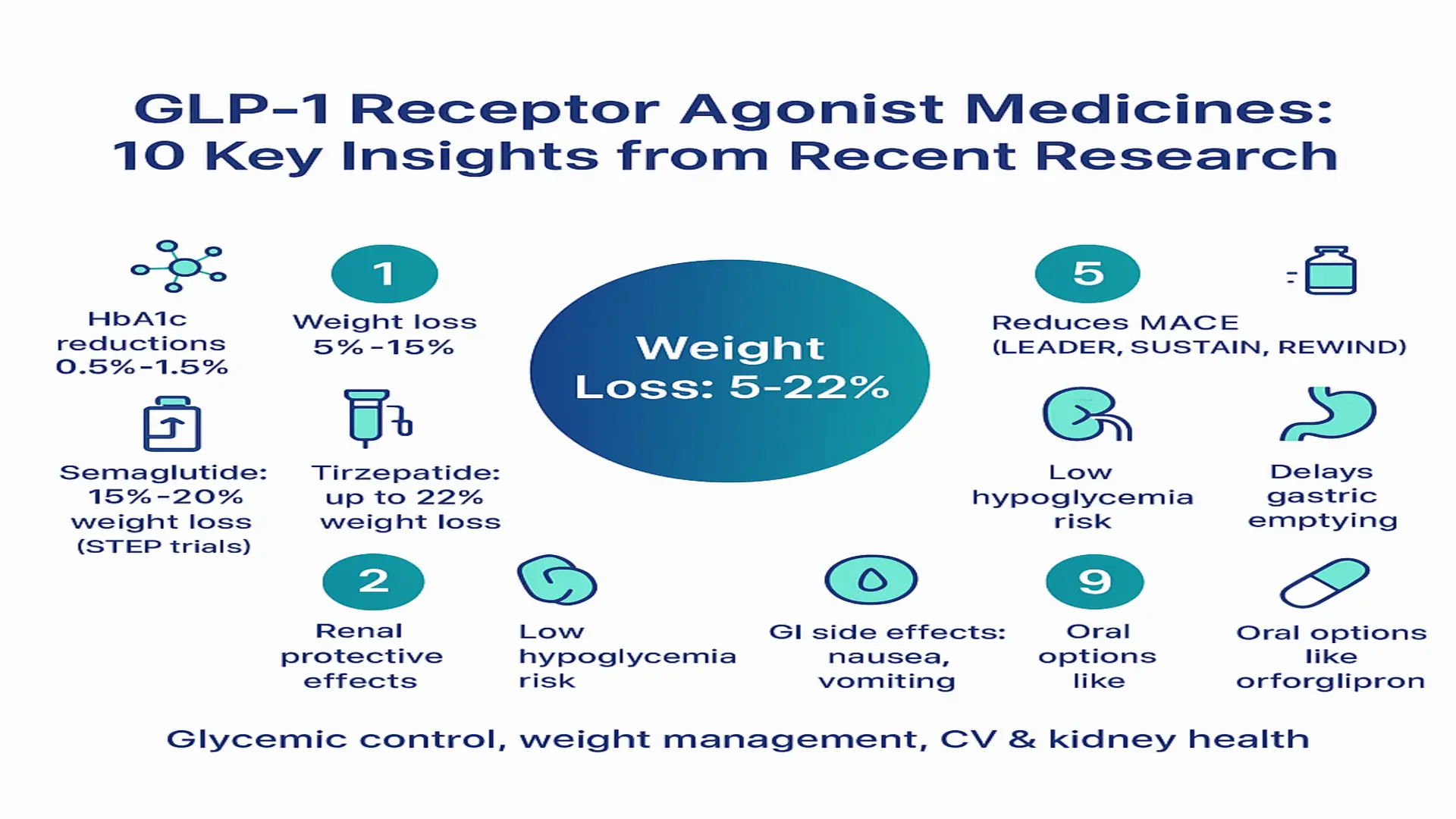
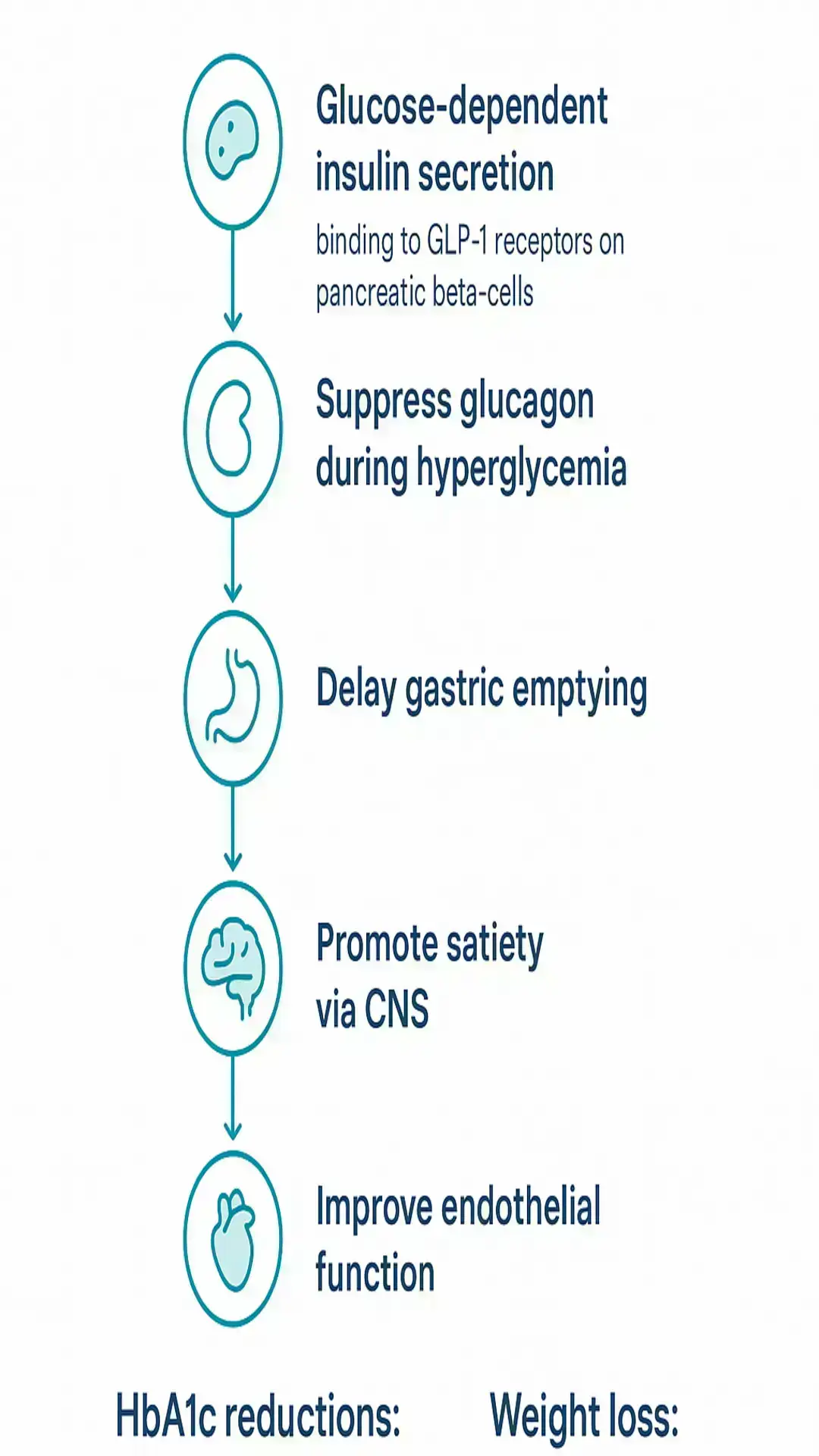
GLP-1 receptor agonist medicines exert their effects by binding to GLP-1 receptors located on pancreatic beta-cells, promoting glucose-dependent insulin secretion. This mechanism helps maintain balanced insulin release without significantly increasing hypoglycemia risk during normal glucose levels. They also suppress glucagon release from alpha-cells specifically during periods of hyperglycemia, contributing to improved glucose regulation.
Additional actions include delaying gastric emptying, which can promote a sense of satiety through central nervous system pathways that regulate appetite. These medicines influence food intake via hypothalamic modulation and interactions with peripheral gut hormones. Research further indicates enhancements in insulin sensitivity and potential cardiovascular benefits through improved endothelial function.
Dual and triple agonists, such as tirzepatide (GLP-1/GIP) or those incorporating glucagon receptor activation, offer enhanced effects on weight management and metabolic flexibility. These multi-receptor approaches aim to amplify satiety signals while preserving lean mass and supporting energy expenditure.
These statements have not been evaluated by the Food and Drug Administration. These mechanisms are supported by research and not intended to diagnose, treat, cure, or prevent any disease.
Therapeutic Applications
GLP-1 receptor agonist medicines are primarily researched for their contributions to HbA1c reduction and weight management in T2D. They have received approvals for obesity treatment in overweight or obese adults without diabetes, including agents like semaglutide and liraglutide. Studies also explore their role in cardiovascular risk reduction among T2D patients with established conditions.
Emerging research points to renal protective effects, such as slowing the progression of chronic kidney disease in relevant populations. Other areas of investigation include prediabetes, heart failure, and non-alcoholic steatohepatitis (NASH). These applications underscore the broadening scope of GLP-1 RAs in metabolic and organ health research, with clinical trials providing foundational evidence for their use.
Clinical Evidence
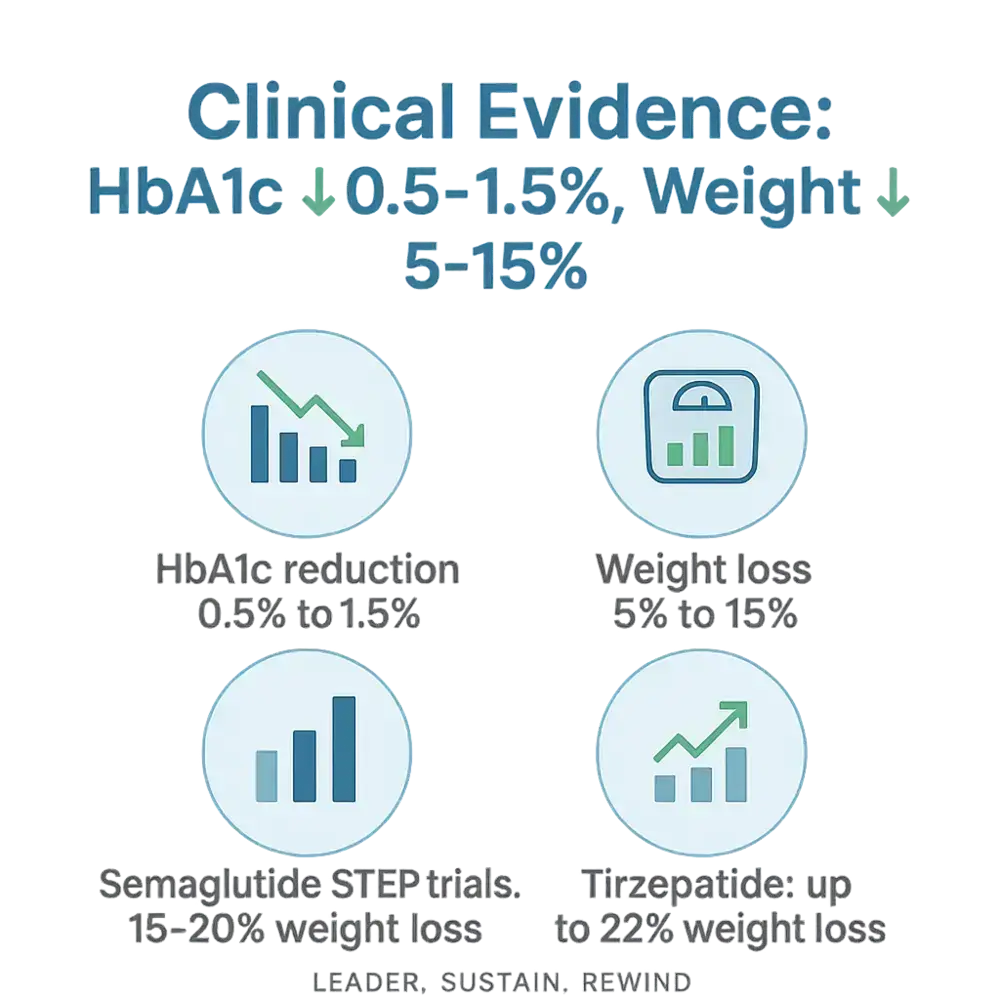
Meta-analyses of GLP-1 receptor agonist medicines demonstrate reductions in HbA1c ranging from 0.5% to 1.5% and body weight decreases of 5% to 15%, accompanied by a low risk of hypoglycemia. Cardiovascular outcome trials, such as LEADER (liraglutide), SUSTAIN (semaglutide), and REWIND (dulaglutide), have shown reductions in major adverse cardiovascular events (MACE) in T2D populations.
The STEP trials for semaglutide in obesity reported weight reductions of 15% to 20% over 68 weeks. Tirzepatide has demonstrated superior outcomes, with up to 22% weight loss and better glycemic control compared to GLP-1 monotherapy in head-to-head studies. Oral GLP-1 RAs like orforglipron have shown promising weight reductions in phase 2 and 3 trials for obesity and T2D, offering potential alternatives to injectables.
These findings are supported by comprehensive evaluations, including network meta-analyses that rank GLP-1 RAs highly for efficacy and safety profiles relative to other therapies.
Challenges and Limitations
While GLP-1 receptor agonist medicines offer notable benefits, they are associated with common gastrointestinal side effects, including nausea, vomiting, diarrhea, and abdominal pain. These effects are often dose-dependent and transient, improving with continued use or dose titration. Rare but serious risks include pancreatitis, gallbladder-related issues, and non-arteritic anterior ischemic optic neuropathy (NAION).
Other limitations involve weight regain after discontinuation and potential loss of lean mass during treatment, highlighting the need for lifestyle integration. Contraindications include a history of medullary thyroid carcinoma or severe gastroparesis. Access barriers such as high costs, the need for injections, and supply shortages further complicate widespread use. Ongoing monitoring and patient education are essential to manage these challenges effectively.
Future Directions
The pipeline for GLP-1 receptor agonist medicines includes oral small-molecule options like orforglipron, which could simplify administration and improve adherence. Dual agonists (GLP-1/GIP) and triple agonists (GLP-1/GIP/glucagon) are in development to enhance efficacy in weight management and metabolic outcomes.
Long-term studies are investigating neuropsychiatric effects, potential suicidality signals, and expanded indications such as Alzheimer’s disease and addiction. Research also focuses on combination therapies to counteract muscle loss, sustain weight management, and optimize dosing. Economic analyses, real-world adherence data, and personalized medicine approaches will shape future guidelines and accessibility.
Conclusion
GLP-1 receptor agonist medicines stand out in research for their evidence-based roles in glycemic control, weight management, and cardiovascular and renal health support in T2D and obesity contexts. Clinical trials affirm their efficacy and generally favorable safety profiles compared to alternatives. While gastrointestinal tolerability poses the main challenge, with rare risks under scrutiny, innovations like dual/triple agonists and oral formulations signal expanded potential. Continued research will refine their integration into metabolic health strategies.
References
- Ghusn W et al. Weight loss outcomes, tolerability, side effects, and risks associated with GLP-1RAs. PMC11404059, 2024
- Latif W. Compare and Contrast the Glucagon-Like Peptide-1 Receptor Agonists. NBK572151, 2024
- Comprehensive evaluation of GLP-1 receptor agonists. Nature Communications, 2025
- Sheth K et al. The expanding scope of GLP-1 receptor agonists. PMC12590185, 2025
- GLP-1 single, dual, and triple receptor agonists for treating type 2 diabetes and obesity. eClinicalMedicine, 2024
- Moiz A et al. The expanding role of GLP-1 receptor agonists. PMC12303005, 2025
- Ansari HUH et al. Efficacy and Safety of Glucagon-Like Peptide-1 Receptor Agonists. PubMed 38029929, 2024
- Mechanisms of GLP-1 Receptor Agonist-Induced Weight Loss. American Journal of Medicine, 2025
- Mechanisms of action and therapeutic applications of GLP-1 and GIP receptor agonists. Frontiers in Endocrinology, 2024
- Glucagon-Like Peptide-1 Receptor Agonists. StatPearls NBK551568
- Exploring the Side Effects of GLP-1 Receptor Agonist. Diabetes Metab J, 2024
- The expanding role of GLP-1 receptor agonists: a narrative review. eClinicalMedicine, 2025
References
References
- Ghusn W et al. Weight loss outcomes, tolerability, side effects, and risks associated with GLP-1RAs. PMC11404059, 2024
- Latif W. Compare and Contrast the Glucagon-Like Peptide-1 Receptor Agonists. NBK572151, 2024
- Comprehensive evaluation of GLP-1 receptor agonists. Nature Communications, 2025
- Sheth K et al. The expanding scope of GLP-1 receptor agonists. PMC12590185, 2025
- GLP-1 single, dual, and triple receptor agonists for treating type 2 diabetes and obesity. eClinicalMedicine, 2024
- Moiz A et al. The expanding role of GLP-1 receptor agonists. PMC12303005, 2025
- Ansari HUH et al. Efficacy and Safety of Glucagon-Like Peptide-1 Receptor Agonists. PubMed 38029929, 2024
- Mechanisms of GLP-1 Receptor Agonist-Induced Weight Loss. American Journal of Medicine, 2025
- Mechanisms of action and therapeutic applications of GLP-1 and GIP receptor agonists. Frontiers in Endocrinology, 2024
- Glucagon-Like Peptide-1 Receptor Agonists. StatPearls NBK551568
- Exploring the Side Effects of GLP-1 Receptor Agonist. Diabetes Metab J, 2024
- The expanding role of GLP-1 receptor agonists: a narrative review. eClinicalMedicine, 2025